Discoid lateral meniscus
Images

Discoid lateral meniscus
Findings
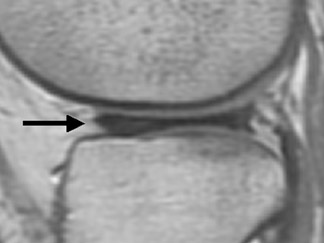
Magnetic resonance imaging (MRI) revealed an elongated free edge of the diffusely enlarged lateral meniscus extending toward the intercondylar region on coronal T1-weighted images (Figure 1A). Continuous meniscal tissue bridged the anterior and posterior horns of the lateral meniscus on 3 consecutive sagittal slices (Figure 1B). The intrameniscal signal in the anterior horn was compatible with mucinous degeneration.
Discussion
Discoid lateral meniscus is a congenital condition that is estimated to occur in 4% to 5% of the population1-4 but has been shown to be as high as 13% in Asian populations.5 It is the most common abnormal meniscal variant in children.6 The condition is typically asymptomatic and, therefore, is infrequently diagnosed.7 The most frequent symptom is pain that usually begins with a minor trauma. Other symptoms include clicking, snapping, clunking, and locking during movement, as well as joint-line tenderness, reduced mobility, and “giving-way.”6,8,9 A high percentage of cases present with an associated meniscal tear and peripheral rim instability.4,9,10 Although discoid lateral meniscus is commonly bilateral, symptoms tend to occur on one side.8
Discoid lateral meniscus is traditionally classified as one of 3 types based on those described by Watanabe et al.11 The complete type refers to complete meniscal coverage of the tibial plateau, while the incomplete type covers <80% of the tibial plateau. The Wrisberg ligament type refers to a more normal morphology, except for a thick posterior horn and a lack of posterolateral meniscotibial attachment, and has a thick posterior tibial attachment.2,3,6 Newer classifications based on shape, stability, tear pattern, and symptoms have been proposed because classification and surgical outcomes have been associated with meniscal tear patterns and lateral compartment changes.12,13
The etiology of discoid lateral meniscus is still debatable, although opinions in the literature tend toward a congenital origin. The reports of additional anatomic variations complicate the original etiology theories and support the concept that discoid lateral meniscus may be due to multiple etiologies.
The most prominent distinguishing features of discoid lateral meniscus on plain radiographs include widening of the lateral joint space and a high fibular head.12,14,15 Additionally, marginal osteophytes and cupping or flattening of the lateral tibial plateau may be revealed.15 MRI has been shown to be effective in the diagnosis of discoid lateral meniscus. Any of the following factors have been shown to be specific for diagnosis: 1) 14- to 15-mm minimum transverse width of the lateral meniscus on a central coronal image. Normally, the meniscus measures 5 to 13 mm; 2) 20% for the ratio of the meniscus to the tibia; and 3) 75% for the ratio of the sum of the width of the anterior and posterior horns to the meniscal diameter on a sagittal slice that shows a maximum meniscal diameter. Contiguous body segment appearance must be shown on 3 consecutive sagittal 4- to 5-mm thick slices.16,17 MRI may also help identify specific types of meniscal tears.18
The most commonly practiced treatment for stable, complete, or incomplete types of discoid lateral meniscus is partial meniscal excision. In this case, our patient underwent surgical excision, leaving a 6- to 7-mm peripheral rim circumferentially, anteriorly, and posteriorly. Postsurgically, the patient continued to have pain and decreased extension of the knee. She had to undergo a second knee arthroscopy to remove more of the meniscus and remaining scar tissue. The patient is now doing well and currently reports no pain or limitation in movement.
CONCLUSION
The diagnosis of discoid lateral meniscus is easily rendered on MRI. Invasive surgical treatment for discoid lateral meniscus is effective for symptomatic relief but is recommended only if the symptoms of the condition become significantly problematic.
- Dickhaut SC, DeLee JC. The discoid lateral-meniscus syndrome. J Bone Joint Surg Am. 1982; 64:1068-1073.
- Kocher MS, Klingele K, Rassman SO. Meniscal disorders: Normal, discoid, and cysts. Orthop Clin North Am. 2003;34:329-340.
- Neuschwander DC, Drez D Jr, Finney TP. Lateral meniscal variant with absence of the posterior coronary ligament. J Bone Joint Surg Am. 1992;74:1186-1190.
- Rohren EM, Kosarek FJ, Helms CA. Discoid lateral meniscus and the frequency of meniscal tears. Skeletal Radiol. 2001;30:316-320.
- Fukuta S, Masaki K, Korai F. Prevalence of abnormal findings in magnetic resonance images of asymptomatic knees. J Orthop Sci. 2002;7:287-291.
- Kelly BT, Green DW. Discoid lateral meniscus in children. Curr Opin Pediatr. 2002;14:54-61.
- Davidson D, Letts M, Glasgow R. Discoid meniscus in children: Treatment and outcome. Can J Surg. 2003;46:350-358.
- Connolly B, Babyn PS, Wright JG, Thorner PS. Discoid meniscus in children: Magnetic resonance imaging characteristics. Can Assoc Radiol J. 1996;47:347-354.
- Rao PS, Rao SK, Paul R. Clinical, radiologic, and arthroscopic assessment of discoid lateral meniscus. Arthroscopy. 2001;17:275-277.
- Klingele KE, Kocher MS, Hresko MT, et al. Discoid lateral meniscus: Prevalence of peripheral rim instability. J Pediatr Orthop. 2004; 24:79-82.
- Watanabe M, Takada S, Ikeuchi H. Atlas of Arthroscopy. Tokyo, Japan:Igaku-Shoin;1969.
- Asik M, Sen C, Taser OF, et al. Discoid lateral meniscus: Diagnosis and results of arthroscopic treatment. Knee Surg Sports Traumatol Arthrosc. 2003;11:99-104.
- Bin SI, Kim JC, Kim JM, et al. Correlation between type of discoid lateral menisci and tear pattern. Knee Surg Sports Traumatol Arthrosc. 2002;10:218-222.
- Kim SJ, Moon SH, Shin SJ. Radiographic knee dimensions in discoid lateral meniscus: Comparison with normal control. Arthroscopy. 2000;16:511-516.
- Nawata K, Teshima R, Ohno M, et al. Discoid lateral menisci in older patients. A radiographic study of 21 cases. Int Orthop. 1999;23:232-235.
- Araki Y, Yamamoto H, Nakamura H, Tsukaguchi I. MR diagnosis of discoid lateral menisci of the knee. Eur J Radiol. 1994;18:92-95.
- Samoto N, Kozuma M, Tokuhisa T, Kobayashi K. Diagnosis of discoid lateral meniscus of the knee on MR imaging. Magn Reson Imaging. 2002; 20:59-64.
- Chiang H, Jiang CC. Discoid lateral meniscus: Clinical manifestations and arthroscopic treatment. J Formos Med Assoc. 2003;102: 17-22.
Related Articles
Citation
. Discoid lateral meniscus. Appl Radiol.
June 13, 2008