Spironolactone-induced gynecomastia
Images
Spironolactone-induced gynecomastia
Findings
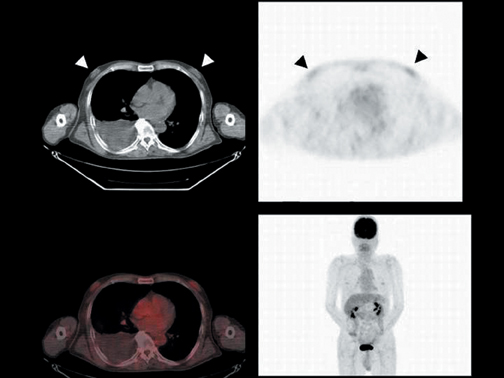
Proliferated bilateral mammary tissue was demonstrated on CT (Figure 1, upper
left), while increased FDG uptake in the bilateral anterior chest was observed on FDG-PET (SUVmax = 2.3, Figure 1, upper right), and the anatomical localization of FDG uptake in the mammary tissue was confirmed by co-registration of the FDG-PET and CT images (Figure 1, lower left).
Discussion
Reports of physiological uptake of FDG in many organs have been increasing with the growing frequency of FDG-PET examinations. In mammary tissue, physiological uptake, uptake in benign tumors, and mastopathy have been also reported.1
Gynecomastia is a common clinical condition consisting of a benign proliferation of male breast glandular tissue;2 its representative symptom is pain and swelling of the breast. Gynecomastia itself is not a disease but, rather, a symptom of an underlying imbalance in hormonal physiology—specifically, an increase in estrogen action relative to androgen action at the breast tissue level.3,4 Transient gynecomastia occurs in the neonatal, pubertal, and senescent periods, and some drugs and disease states are also known causes of gynecomastia.3-5
Spironolactone is a potassium-holding diuretic used to treat ascites due to liver cirrhosis, and gynecomastia is a well-known side effect of the medication. Rose, et al., reported that 6 of 16 patients treated with spironolactone developed gynecomastia.6 According to this report,blood testosterone levels were lower and estradiol levels higher in the gynecomastia group than they were in the control group, indicating the disturbance in hormone balance with estrogen predominating. The treatment for drug-induced gynecomastia is withdrawal of the causative drug, leading to the disappearance of the symptom. In this case, the patient suffered from liver cirrhosis with ascites, for which spironolactone had been prescribed. Although liver cirrhosis also causes gynecomastia, due to the increase of aromatization, the patient was taken off spironolactone after the FDG-PET/CT examination, and his symptoms disappeared. Therefore, we considered this a case of spironolactone-induced gynecomastia. FDG uptake in spironolactone-induced gynecomastia is also reported by Fukuchi, et al.7
Gynecomastia is observed as a proliferation of breast tissue on CT and as dense breast tissue on mammography. The relationship between breast density and FDG uptake was reported by Vranjesevic, et al.8 FDG uptake in dense breast tissue was significantly higher than that in fatty breast tissue. Uno, et al., compared FDG uptake and ultrasonographic findings in fibrocystic mastopathy patients,1 FDG uptake in mammary tissue correlated with severity of mastopathy. These reports suggest that proliferation of breast tissue causes the increase of FDG uptake. FDG-PET/CT can provide morphological and functional information simultaneously and assess the status of mammary tissue through co-registration of both images.
Conclusion
We reported a case of spironolactone-induced gynecomastia revealed by FDG-PET/CT. In male patients, history of medication and illness should be taken into account when FDG uptake in bilateral mammary tissue is observed.
- Uno K, Yoshikawa K, Imazaki K, et al. FDG-PET evaluation of fibrocystic mastopathy in patient with breast tumor. Eur J Nucl Med. 1994;21:S197.
- Nuttall FQ. Gynecomastia as a physical finding in normal men. J Clin Endocrinol Metab. 1979;48:338-340.
- Glass AR. Gynaecomastia. Endocrinol Metab Clin North Am. 1994;23:825-837.
- Braunstein GD. Gynecomastia. N Engl J Med. 1993;328:490-495.
- Mathur R, Braunstein GD. Gynecomastia: Pathomechanisms and treatment strategies. Horm Res. 1997;48:95-102.
- Rose LI, Underwood RH, Newmark SR, et al. Pathophysiology of spironolactone-induced gynecomastia. Ann Int Med. 1977;87:398-403.
- Fukuchi K, Sasaki H, Yokoya T, et al. Ga-67 citrate and F-18 FDG uptake in spironolactone-induced gynecomastia. Clin Nucl Med. 2005;30:105-106.
- Vranjesevic D, Schiepers C, Silverman DH, et al. Relationship between 18F-FDG uptake and breast density in women with normal breast tissue. J Nucl Med. 2003;44:12381242.