Riedel’s thyroiditis
Images


Case Summary
A 47-year-old man underwent ultrasonography of the thyroid for a neck mass. He had undergone right thyroidectomy and isthmusectomy 10 years earlier for a progressively enlarging thyroid gland. Multiple biopsies from this procedure were negative for malignancy. Preoperatively, thyroid antibodies were negative and, despite levothyroxine sodium therapy (Synthroid, Abbott Laboratories, Abbott Park, IL), thyromegaly progressed. The patient reported difficulty swallowing solid foods but no other compressive symptoms. Pathologic findings were consistent with Riedel's struma, displaying inflammatory fibrosclerosis with hyaline bands of coarse fibrosis. The left thyroid lobe was not explored. Following surgery, the patient noted an improvement in swallowing.
Imaging Findings
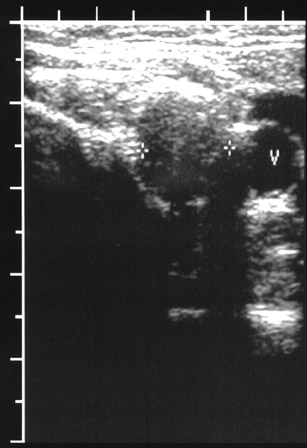
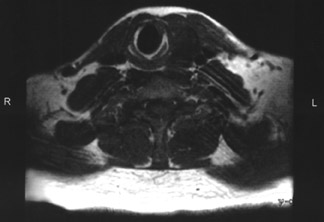
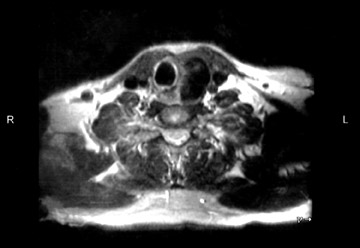
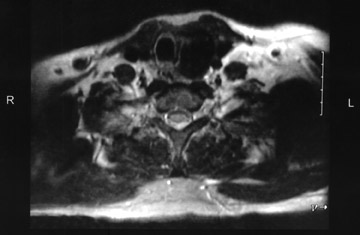
The patient underwent ultrasonography of the neck, which showed a 3-cm hypoechoic mass with posterior shadowing within the lateral aspect of the remaining left thyroid lobe (Figure 1). There was minimal normal thyroid tissue medially. One month later, an I123 thyroid scan was performed at an outside institution that revealed absent uptake on delayed images (not shown). Three months later, magnetic resonance (MR) imaging of the neck was performed (Figure 2). Low signal intensity was present throughout the left lobe on T1-weighted images, with further decreased signal intensity on T2-weighted images. Mild extrinsic impression on the esophagus and tracheal deviation to the right was also found.
Diagnosis
Riedel's thyroiditis
Discussion
Riedel's thyroiditis is a rare entity in which fibrous tissue replaces the thyroid gland and tends to extend into the surrounding tissues.1 It was first described in 1883 by Bernard Riedel.2 In 1957, a study by Beahrs et al3 found Riedel's thyroiditis in 20 of 40,000 thyroidectomies over a period of 36 years, attesting to the rarity of the disease. Hay et al4 found that the overall incidence in the ambulatory setting is 1.06 in 100,000 individuals.
Pathologically, Riedel's thyroiditis is characterized by replacement of normal thyroid tissue by fibrotic connective tissue, with obliteration of normal thyroid architecture and involvement of adjacent tissues following extension through the thyroid capsule. Diffuse or partial involvement of the gland may occur. There is absence of skin and lymph node involvement.1,5 Clinically, the thyroid gland is enlarged and hard but nontender and frequently involves a previously existing goiter.5 Direct extension causes compression of the trachea and the esophagus, resulting in dyspnea and dys-phagia.1,5 An association exists between Riedel's thyroiditis and multifocal idiopathic fibro-sclerosis, which includes retroperitoneal fibrosis, pseudo-tumor of the orbit, sclerosing cholangitis, and mediastinal fibrosis.6,7
The exact etiology is still unknown.1 Although it was previously thought to represent the later stages of Hashimoto's thyroiditis, Riedel's thyroiditis is now recognized as a unique disease process.5 Early lesions show inflammatory cell infiltration with destruction of normal thyroid architecture. Ensuing fibrosis replaces normal thyroid tissue and is not confined to the thyroid gland.1,8 Thyroid function is typically preserved until later stages when patients exhibit hypothyroidism, which can also occur from fibrotic infiltration of the parathyroid glands.
In a review of cases of Riedel's thyroiditis reported in the literature, Schwaegerle et al8 found that the majority of patients were euthyroid, predominantly female, and had a wide age range of 23 to 77 years. Wedge resection is required for tissue diagnosis; fine needle aspiration does not provide adequate tissue.5 Our patient was described to have had multiple biopsies before thyroidectomy, showing neither evidence of malignancy nor evidence of Riedel's thyroiditis. The natural history of Riedel's thyroiditis is most likely self-limiting; however, treatment can include steroids, as well as surgical excision of all or part of the gland to alleviate compressive symptoms.5,9
Ultrasound can demonstrate a hypoechoic, hypodense mass replacing normal thyroid tissue with extension into adjacent musculature.10 Scintigraphic findings in Riedel's thyroiditis indicate an irregular thyroid gland with low radioiodine uptake, specifically with later stages of the dis-ease.11 The patient's I123 scan performed after right thyroid lobectomy and isthmusectomy revealed no activity on delayed images. MR findings are those characteristic of fibrosis: hypointense signal intensity on T1- and T2-weighted images. There can be contrast enhancement with gadolinium. This is contrasted with most other conditions, including thyroid carcinoma, lymphoma, and Hashimoto's thyroiditis, where there is increased signal intensity on T2-weighted images.10
Conclusion
Riedel's thyroiditis is a rare fibrotic process involving the thyroid gland and surrounding soft tissues. The imaging appearance, as typified by this case, reflects the fibrosis. The lesion can be expected to be hypoechoic, with poor through transmission, on ultrasonography and to have low uptake on scintigraphy and low signal on T1- and T2-weighted MR sequences.