Part 3: Classic signs in gastrointestinal radiology
Images
















Dr. Baldwin is a Radiologist at South Shore Hospital, Weymouth, MA; Dr. Genant is an Associate Professor of Radiology at San Francisco Medical Center, San Francisco, CA; Dr. Braver is the Director of Gastrointestinal Radiology at Brigham & Women’s Hospital and an Assistant Professor at Harvard Medical School, Boston, MA; and Dr. Mortele is the Director of the Division of Clinical MRI at Beth Israel Deaconess Medical Center, Boston, MA, and the Associate Professor of Radiology at Harvard Medical School, Boston, MA.
The names of many classic radiologic signs derive from analogues to objects commonly encountered in everyday life; eg, the “comb” sign. The use of familiar objects to describe visual findings enables radiologists both to arrive at a correct diagnosis and to effectively convey such diagnostic findings to clinicians.
Ring sign
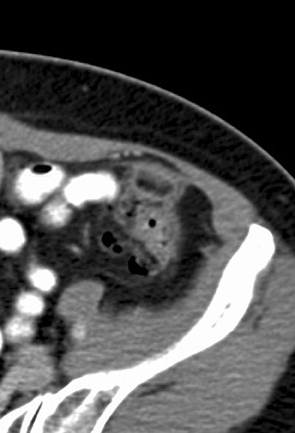
The appendages epiploicae are peritoneal pouches containing pericolonic fat connected to the serosal surface of the colon by a vascular stalk composed of 2 feeding arteries and one draining vein. These appendages are found in 2 rows. One row is medial to the tenia libera; the other lateral to the tenia omentalis. Torsion of the appendages epiploicae with resulting vascular occlusion is believed to be the cause of epiploic appendagitis. The most common sites for epiploic appendagitis are adjacent to the sigmoid colon, descending colon, and right hemicolon.74
The hyperattenuation “ring sign” is a classic finding on CT examinations in epiploic appendagitis. It consists of a thin, round, or oval high-attenuation ring representing thickened, inflamed visceral peritoneum surrounding the torsed epiploic appendage (Figure 26).75 Internally, the high-attenuation ring contains fat and often a central dot of high attenuation that represents the thrombosed central vein.76
Coffee bean sign
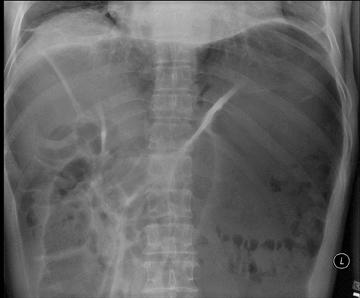
The “coffee bean” sign is seen on supine plain films of the abdomen in approximately 80% of cases of sigmoid volvulus.77 The appearance of the coffee bean is created by the dilated lateral walls of the sigmoid colon forming the outer walls of the coffee bean and the closely apposed medial walls forming the cleft of the coffee bean (Figure 27).78 This gas-filled segment of bowel arises from the pelvis and may fill the entire abdomen. Its apex often extends superior to the 10th thoracic vertebral body and the apex can be located to the left or right of midline.79,80
A cecal volvulus can appear very similar to a sigmoid volvulus; however, a cecal volvulus should have only one air-fluid level, whereas a sigmoid volvulus may demonstrate two air-fluid levels. A distended, transverse colon can also mimic a sigmoid volvulus. This dilated bowel, however, does not arise from within the pelvis and it extends superiorly in a U-shaped configuration.81 The coffee bean sign has also been used to describe small-bowel, closed-loop obstructions.82
Sandwich sign
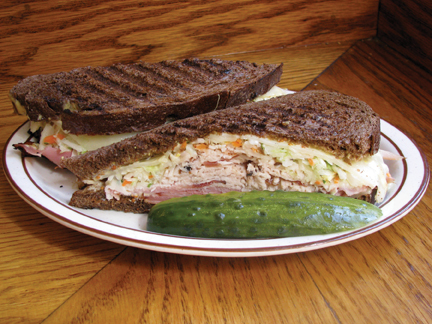
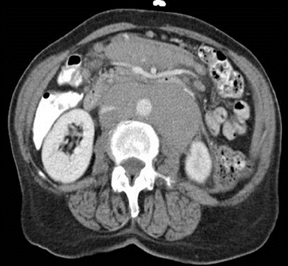
The “sandwich” sign describes the appearance of mesenteric lymphadenopathy encasing enhancing mesenteric vessels and bowel on contrast-enhanced CT studies. The enhancing, encased vascular structures represent the sandwich filling while the soft-tissue attenuation, mesenteric lymphadenopathy comprises the bun (Figure 28). This classic CT sign can also be seen on ultrasound in the presence of mesenteric lymphadenopathy.83
The sandwich sign is specific for mesenteric lymphomas. Although many disease processes may cause mesenteric lymphadenopathy, only lymphoma results in the large, bulky lymphadenopathy that results in the sandwich sign.84
Post-transplantation lymphoproliferative disorder (PTLD) can also cause a sandwich sign in patients who have received solid organ or bone marrow transplants. PTLD is a lymphoproliferation caused by the Ebstein-Barr virus in post-transplant patients.85
Mercedes-Benz sign
This classic plain film finding represents gas-containing fissures within gallstones. Bauer first described this phenomenon in 1931.86 These gas-containing pockets are seen as stellate radiolucencies in the right upper quadrant. The lucencies frequently form a triradiate pattern, thus this finding is referred to as the “Mercedes-Benz” sign (Figure 29).
The radiolucent fissures are most commonly widest centrally and radiate peripherally like the points of a star. Five radiolucent fissures have rarely been observed in gallstones. The radial fissures tend to be of the same length and extend to the mid-point of the sides of faceted stones. They do not extend to the periphery and are mainly located within the central two-thirds of the calculi.87
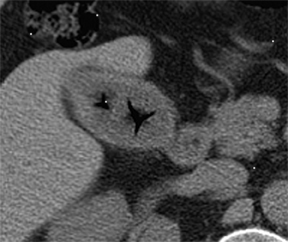
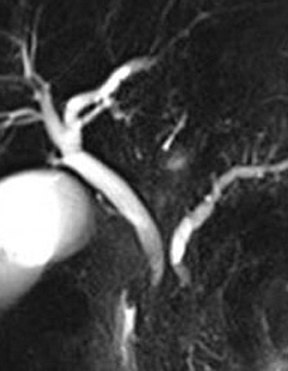
Central dot sign
The “central dot” sign is seen in dilated intrahepatic biliary ducts (IBD). This sign describes the presence of a punctate dot of contrast enhancement within the dilated IBDs. The central dot sign is produced by enhancing branches of the portal vein surrounded by dilated IBDs (Figure 30). This sign is highly suggestive of Caroli disease.88,89
Caroli disease represents the Type V Todani choledochal cyst; communicating cavernous ectasia of the IBDs. It is a rare, autosomal recessive disorder that affects the normal embryologic remodeling of the large intrahepatic ducts. This results in a cystic dilatation of the IBDs. Abnormal development of the small interlobular bile ducts results in congenital hepatic fibrosis. If both the large and small ducts are affected and both features of congenital hepatic fibrosis and Caroli disease are present, this entity is termed Caroli syndrome.90-92
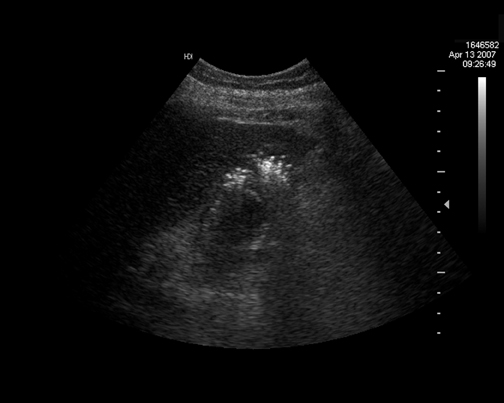
Champagne sign
Hegner first described the radiographic appearance of emphysematous cholecystitis on plain radiographs in 1931.93 This rare form of acute cholecystitis most commonly affects men between the ages of 50 and 70 who have underlying diabetes mellitus and/or atherosclerotic disease.94 Vascular compromise of the cystic artery is thought to play a key role in the etiology of this pathologic process.95
Ultrasonography (US) may show small echogenic foci of gas rising toward the nondependent portion of the gallbladder lumen. These rising foci can mimic the effervescing bubbles one sees in a glass of champagne (Figure 31). The champagne sign is a specific, but insensitive finding in emphysematous cholecystitis. Surrounding pericholecystic gas may obscure the gallbladder lumen from evaluation.96
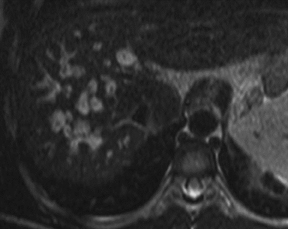
Pearl necklace sign
Adenomyomatosis represents the presence of intramural diverticula of the gallbladder mucosa, the Rokitansky-Aschoff sinuses, within a thickened, hypertrophied mucosa and muscularis propria of the gallbladder wall.97,98
The “pearl necklace” sign was described when the Rokitansky-Aschoff sinuses within the thickened gallbladder wall filled with contrast and opacified during drip-infusion cholecystographic studies, giving a beaded necklace appearance (Figure 32).99 However, successful opacification of the Rokitansky-Aschoff sinuses was seen in only approximately 5% of drip-infusion cholecystograms. The pearl necklace sign is currently much more reliably seen on heavily T2-weighted, fast spin-echo (FSE) magnetic resonance cholangiopancreatography images as a curvilinear arrangement of multiple rounded foci of hyperintense T2 signal within the thickened wall of the gallbladder.100
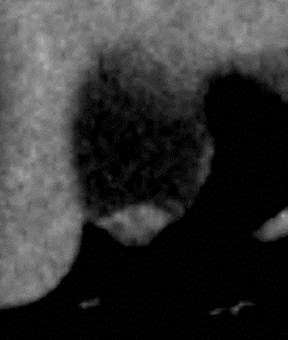
Rosary sign
Adenomyomatosis can also be demonstrated on postcontrast CT images. The “rosary sign” is created on postcontrast CT images by the enhancement of the proliferative mucosal epithelium lining the Rokitansky-Aschoff sinuses surrounded by the unenhanced, hypertrophied muscularis layer of the gallbladder wall.101 The enhancement of multiple, rounded sinuses within the thickened gallbladder wall produces the rosary bead appearance (Figure 33).102
Double duct sign
The “double duct” sign was initially described through the use of endoscopic retrograde cholangiopancreatography (ERCP).103 To date, this sign has also been described using magnetic resonance cholangiopancreatography (MRCP), multidetector CT (MDCT), and ultrasound (US).104-107 The double duct represents simultaneous dilatation of the common bile duct and the pancreatic duct occurring secondary to contiguous distal biductal stenosis (Figure 34).108
The causative narrowing of the common bile and pancreatic ducts most commonly occurs due to contiguous obstruction or encasement by a carcinoma of the head of the pancreas or the ampulla of Vater. Other malignant etiologies of biductal dilatation are metastases, lymphoma, and cholangiocarcinoma of the distal common bile duct.109 Various benign etiologies have also demonstrated the double duct sign. These include chronic pancreatitis and ampullary stenosis. Thus, the double duct sign is highly suggestive of, but not specific for, carcinoma of the head of the pancreas.110
Telltale triangle
The “telltale triangle” sign represents a small amount of free intraperitoneal gas observed on supine cross table lateral radiographs of the abdomen. The crosstable lateral view is extremely sensitive for detecting small amounts of pneumoperitoneum because it utilizes horizontal X-ray beams directed tangentially to intraperitoneal collections of free air.111
The base of the telltale triangle sign is classically formed by free air abutting the anterior parietal peritoneum, with the apex of the triangle pointing posteriorly, formed by free air interposed between 2 or more loops of gas-filled bowel adjacent to the anterior abdominal wall (Figure 35).112
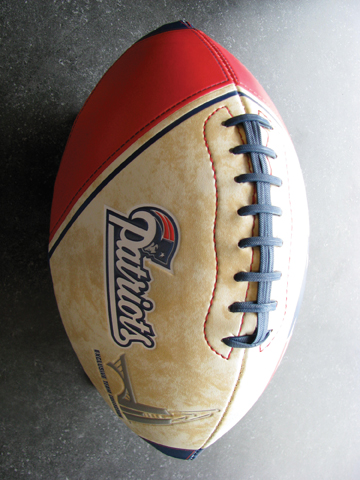
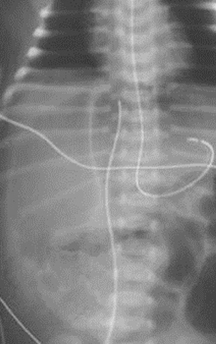
Football sign
Miller first described the “football” sign in 1960.113 This sign represents a large ovoid radiolucency extending in a cephalocaudal axis within the abdomen. The football sign is seen on supine abdominal plain radiographs in severe pneumoperitoneum;114 most frequently in infants with spontaneous or iatrogenic gastric perforation. Only 2% of adults with pneumoperitoneum demonstrate the football sign.115
Abundant free gas within the abdominal cavity collects anterior to the viscera and creates a sharp interface with the parietal peritoneum, thus outlining the peritoneal cavity. This gaseous interface with the peritoneum creates the ovoid shape of an American football (Figure 36). The massive pneumoperitoneum may outline the falciform ligament in the right upper quadrant. The gas may also outline the median umbilical ligament that is composed of the urachal vestige. The medial and lateral umbilical folds may also be outlined. These folds are composed of the umbilical and inferior epigastric vessels, respectively, that form the seams of the football.113,116
Rigler/bas-relief sign
The “Rigler ” or “bas-relief” sign is also seen on supine plain radiographs of the abdomen in cases of pneumoperitoneum. Rigler first described this finding in 1941.117 This sign is seen only in the presence of moderate to large amounts of pneumoperitoneum. With a prevalence of 32%, the bas-relief sign follows right upper-quadrant, subdiaphragmatic free air as the second most common sign of pneumoperitoneum on supine plain radiographs.115
The bas-relief sign represents the visualization of both the luminal and serosal surfaces of the bowel wall due to the accumulation of free intraperitoneal gas between bowel loops (Figure 37).118 A variant of the Rigler sign occurs when only the external surface of the bowel wall is visualized due to the presence of fluid within the bowel lumen.115
The bas-relief sign can be mimicked by two closely contiguous loops of bowel. In this case, intraluminal gas in one loop can appear to outline the wall of an adjacent loop.115 Residual oral contrast from a recent CT study can also increase the apparent bowel-wall attenuation and create a pseudo-Rigler sign.119 Mach bands can also create a false positive bas-relief sign because there is the perception of a line at the interface of two differing radiographic densities.120
Cupola sign
The “cupola sign” represents an inverted cup-shaped lucency seen within the upper abdomen on supine plain radiographs in pneumoperitoneum (Figure 38).121 This arcuate radiographic lucency projects across the midline caudal to the heart in the subxiphoid region.122
The cupola sign represents free intraperitoneal air located within the subphrenic space.123 The subphrenic space is located anterior to the stomach and the gastrohepatic ligament. This space creates a well-defined superior border to the gas collection, thus forming the cupola sign.
The central tendon of the diaphragm forms the well-defined superior margin of the cupola sign. The central tendon is composed of the right, left, and central diaphragmatic leaves. Gas collects below the central leaf, the most anterior portion of the diaphragmatic tendon, when the patient is supine.124
Potential mimickers of the cupola sign can occur with the presence of air within the lesser sac, gas within the high transverse colon, gas within a horizontally-oriented stomach, pneumopericardium, or pneumomediastinum.122
Conclusion
The recognition of classic radiologic signs that resemble familiar real-world objects can be helpful in diagnosis. These signs result directly from the underlying pathophysiology associated with either a single or a well-defined group of entities. Appreciation of these “objects” in a background of more complex and potentially confusing imaging findings will assist in reaching an accurate diagnosis or assist in selection of additional studies to narrow the diagnostic possibilities.
References
- . Singh AK, Gervais DA, Hahn PF, et al. Acute epiploic appendagitis and its mimics. Radiographics. 2005;25:1521-1534.
- van Breda Vriesman AC. The hyperattenuating ring sign. Radiology. 2003;226:556-557.
- Rioux M, Langis P. Primary epiploic appendagitis: Clinical, US, and CT findings in 14 cases. Radiology. 1994;191:523-526.
- Jones IT, Fazio VW. Colonic volvulus: Etiology and management. Dig Dis. 1989;7:203-209.
- Feldman D. The coffee bean sign. Radiology.2000;216:178-179.
- Burrell HC, Baker DM, Wardrop P, Evans AJ. Significant plain film findings in sigmoid volvulus. Clin Radiol.1994;49:317-319.
- Young WS, Engelbrecht HE, Stroker A. Plain film analysis in sigmoid volvulus. Clin Radiol.1978;29:553-560.
- Margulis AR, Burhenne HJ, eds. In: Alimentary tract radiology. 4th ed. St Louis, Mo: Mosby;1989:338, 345-350.
- Mellins Z, Riger LG. The roentgen findings in strangulating obstructions of the small intestine. Am J Gastroenterol.1954;71:404-415.
- Mueller PR, Ferrucci JT, Harbin WP, et al. Appearance of lymphomatous involvement of the mesentery by ultrasonography and body computed tomography: The “sandwich sign.” Radiology. 1980;134:467-473.
- Hardy SM. The sandwich sign. Radiology. 2003;226:651-652.
- Swinnen LJ. Overview of posttransplant b-cell lymphoproliferative disorders. Semin Oncol. 1999;26:21-25.
- Bauer KH. Uber selbstzertrummerung von galensteinen und neubildung von steinen auf der grundlage von steintrummern. Arch Klin Chir. 1931;165:53-80.
- Meyers MA, O’Donohue N. gallstones. The Mercedes-Benz sign: Insight into the dynamics of formation and disappearance of gallstones. Am J Gastroenterol.1973;119:63-70.
- Choi BI, Yeon KM, Kim SH, Han MC. Caroli disease: Central dot sign in CT. Radiology. 1990;174:161-163.
- Mortele KJ, Rocha TC, Streeter JL, Taylor AJ. Multimodality imaging of pancreatic and biliary congenital anomalies. Radiographics. 2006;3:715-731.
- Mortele KJ, Ros PR. Cystic focal liver lesions in the adult: Differential CT and MR imaging features. Radiographics. 2001;21:895-910.
- Levy AD, Rohrmann Jr CA, Murakata LA, Lonergan GJ. Caroli’s disease: Radiologic spectrum with pathologic correlation. Am J Gastroenterol.2002;179:1053-1057.
- Harjai MM, Bal RK. Caroli syndrome. Pediatr Surg Int. 2000;16:431-432.
- Hegner CF. Gaseous pericholecystitis with cholecystitis and cholelithiasis. Arch Surg. 1931;22:993-1000.
- Grayson DE, Abbott RM, Levy AD, Sherman PM. Emphysematous infections of the abdomen and pelvis: A pictorial review. Radiographics. 2002;22:543-561.
- Jolly BT, Love JN. Emphysematous cholecystitis in an elderly woman: Case report and review of the literature. J Emerg Med. 1993;11:593-597.
- Wu CS, Yao WJ, Hsiao CH. Effervescent gallbladder: A sonographic finding in emphysematous cholecystitis. J Clin Ultrasound. 1998;26:272-275.
- Colqunhoun J. Adenomyomatosis of the gall-bladder (intramural diverticulosis). Br J Radiol.1961;34:101-112.
- Williams I, Slavin G, Cox AG. Diverticular disease (adenomyomatosis) of the gallbladder: A radiological-pathological survey. Br J Radiol.1986;59:29-34.
- Dahnert W. Radiology Review Manual. 4th Ed. Baltimore, Md: Williams & Wilkins;1999:593.
- Haradome H, Ichikawa T, Sou H, et al. The pearl necklace sign: An imaging sign of adenomyomatosis of the gallbladder at mr cholangiopancreatography. Radiology. 2003;227:80-88.
- Chao C, Hsiao HC, Wu CS, Wang KC. Computed tomographic finding in adenomyomatosis of the gallbladder. J Formos Med Assoc. 1992;91:467-469.
- Boscak AR, Al-Hawary M, Ramsburgh SR. Best cases from the AFIP: Adenomyomatosis of the gallbladder. Radiographics. 2006;26:941-946.
- Ralls PW, Halls J, Renner, I, Juttner H. Endoscopic retrograde cholangiopancreatography (ERCP) in pancreatic disease: A reassessment of the specificity of ductal abnormalities in differentiating benign from malignant disease. Radiology. 1980;134:347-352.
- Nino-Murcia M, Jeffrey RB, Beauliu CF, et al. Multidetector CT of the pancreas and bile duct system: Value of curved planar reformations. Am J Gastroenterol. 2001;176:689-693.
- Blangy S, Cornud F, Breil JL, et al. Value of ultrasonography in the diagnosis of carcinoma of vater’s ampulla: Apropos of 9 cases. J Radiol.1986;67:335-339.
- Ahualli J. The double duct sign. Radiology. 2007;244:314-315.
- Sahni VA, Mortele KJ. Magnetic resonance cholangiopancreatography: Current use and future applications. Clin Gastroenterol Hepatol. 2008;6:967-977.
- Soto JA, Alvarez O, Lopera JE et al. Biliary obstruction: Findings at MR cholangiography and cross sectional MR imaging. Radiographics. 2000;20:353-366.
- Baillie J, Paulson E, Vitellas K. Biliary imaging: A review. Gastroenterology. 2003;124:1686-1699.
- Kalady MF, Peterson B, Baillie J, et al. Pancreatic duct strictures: Identifying risk of malignancy. Ann Surg Oncol. 2004;11:581-588.
- Epelman M, Daneman A, Navarro OM, et al. Necrotizing enterocolitis: Review of state-of-the-art imaging findings with pathologic correlation. Radiographics. 2007;27:285-305.
- Seibert JJ, Parvey LS. The telltale triangle: Use of the supine cross table lateral radiograph of the abdomen in early detection of pneumoperitoneum. Pediatr Radiol. 1977;5:209-210.
- Miller RE. Perforated viscus in infants: A new roentgen sign. Radiology. 1960;74:65-67.
- Rampton JW. The football sign. Radiology. 2004;231:81-82.
- Levine MS, Scheiner JD, Rubesin SE, et al. Diagnosis of pneumoperitoneum on supine abdominal radiographics. Am J Gastroenterol.1991;156:731-735.
- Kirks DR, Griscom NT, eds. In: Practical Pediatric Imaging: Diagnostic Radiology of Infants and Children. 3rd ed. Philadelphia, Pa: Lippincott-Raven; 1998:890-893.
- Rigler LG. Spontaneous pneumoperitoneum: A roentgenologic sign found in the supine position. Radiology.1941;37:604-607.
- Ly JQ. The rigler sign. Radiology. 2003;228: 706-707.
- Baker SR, Cho KC, eds. In: The abdominal plain film with correlating imaging. Stanford, Conn.: Appleton & Lange; 1999:118-122.
- Chasen MH. Practical applications of Mach band theory in thoracic analysis. Radiology. 2001;219:596-610.
- Mindelzun RE, McCort JJ. The cupola sign of pneumoperitoneum in the supine patient. Gastrointest Radiol. 1986;11:283-285.
- Marshall GB. The cupola sign. Radiology. 2006;241:623-624.
- In: Meyers M. Dynamic Radiology of the Abdomen. 5th ed. New York, NY: Springer-Verlag, 2000:319-320.
- In: Grant JC, Agur AM, Ming JL, Anderson JE. Grant’s Atlas of Anatomy. 9th ed. Baltimore, Md: Williams & Wilkins, 1991;137.