Ganglioglioma
Images
Prepared by Iman Naseri, MD, Resident, Otolaryngology Head and Neck Surgery, Emory University, Atlanta, GA; and Ranjiv K Saini, MD, Assistant Professor of Radiology, and Cynthia T. Welsh, MD, Assistant Professor of Pathology and Laboratory Medicine, Medical University of South Carolina, Charleston, SC.
CASE SUMMARY
A 10-year-old white boy presented with a 2-year history of staring spells and automatisms followed by 10 to 20 minutes of sleep. He had an unremarkable medical history other than an existing seizure disorder. Medications included divalproex sodium (125 mg, 3 tablets po TID) and levetiracetam (250 mg, 2 tablets po TID). Family history was negative for any central nervous system disorders. The patient was in the fifth grade, lived at home with his parents, and had two healthy siblings. He was allergic to lamotrigine, which gave him a generalized rash. His vital signs were: temperature 97.5¢ª, pulse 91 bpm, blood pressure 124/71 mm Hg, and weight 39.7 kg. Physical examination revealed no abnormal findings, and the neurologic examination was normal.
DIAGNOSIS
Ganglioglioma
IMAGING FINDINGS
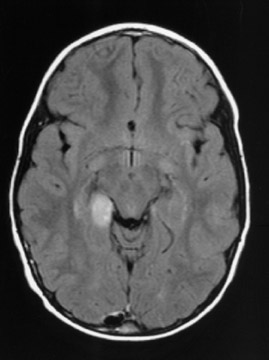
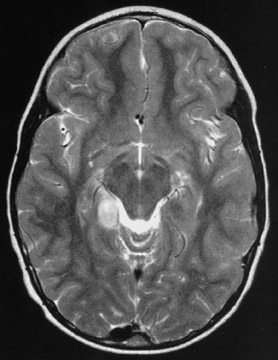
Contrast-enhanced magnetic resonance imaging is the preferred imaging technique to diagnose ganglio-glioma, as it shows signal intensity on T1-weighted images, and high intensity on T2-weighted images. In the images in this case, the tumor presents as a well-defined cystic mass with a solid mural nodule (Figures 1 and 2). These tumors usually reveal iodine or gado-linium enhancement. On computed tomography, these tumors are well-circumscribed and peripherally located. Surrounding edema and hemorrhage is rarely seen. Most images are hypo- or isodense to brain parenchyma with poor contrast. Nuclear imaging and angiography are not helpful in diagnosis.
DISCUSSION
Gangliogliomas are mixed-cell tumors containing both neural ganglionic and glial cell components. They occur often in patients <30 years of age and constitute 0.4% to 7.6% of all brain tumors and approximately 10% of all primary brain tumors in children. 1 It has been difficult to assign such rare tumors to a particular category, as they comprise neuronal and glial precursors derived from the embryonic neuroepithelium. Although they are considered nonaggressive and are slow-growing, gangliogliomas can cause long-standing progressive symptoms that include seizures, symptoms of hydrocephalus, ataxia (if in cerebellum), and headaches. 2 All imaging techniques are nonspecific, but they aid in the definition and localization of the tumor. Therefore, diagnosis is typically established histologically. 3
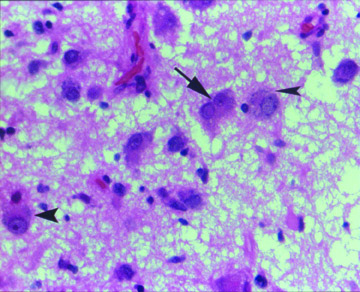
This particular patient had a right craniotomy and resection of the tumor. Histopathology of the brain lesion was found to be a low-grade ganglioglioma (Figure 3). The prognosis is usually excellent if these tumors are fully resected.
CONCLUSION
Although gangliogliomas are rare in the differential diagnosis of intracranial masses, they should be considered in the presence of a well-defined cystic mass in the temporal lobes or cerebellum.