Jejunal Atresia
By Lee JK, Son JK, Spevak MR


Case Summary
An infant born at 35 weeks’ gestational age was diagnosed prenatally with small bowel obstruction via ultrasonography and fetal magnetic resonance imaging (MRI). Given the bowel obstruction and significant output of bilious fluid, a nasogastric tube was placed shortly after birth. At day 2 of life, the infant underwent a fluoroscopic upper gastrointestinal (UGI) series with small-bowel follow through (SBFT). A genetic workup and a complete abdominal ultrasound were also performed to evaluate for other anomalies prior to surgical repair.
Imaging Findings
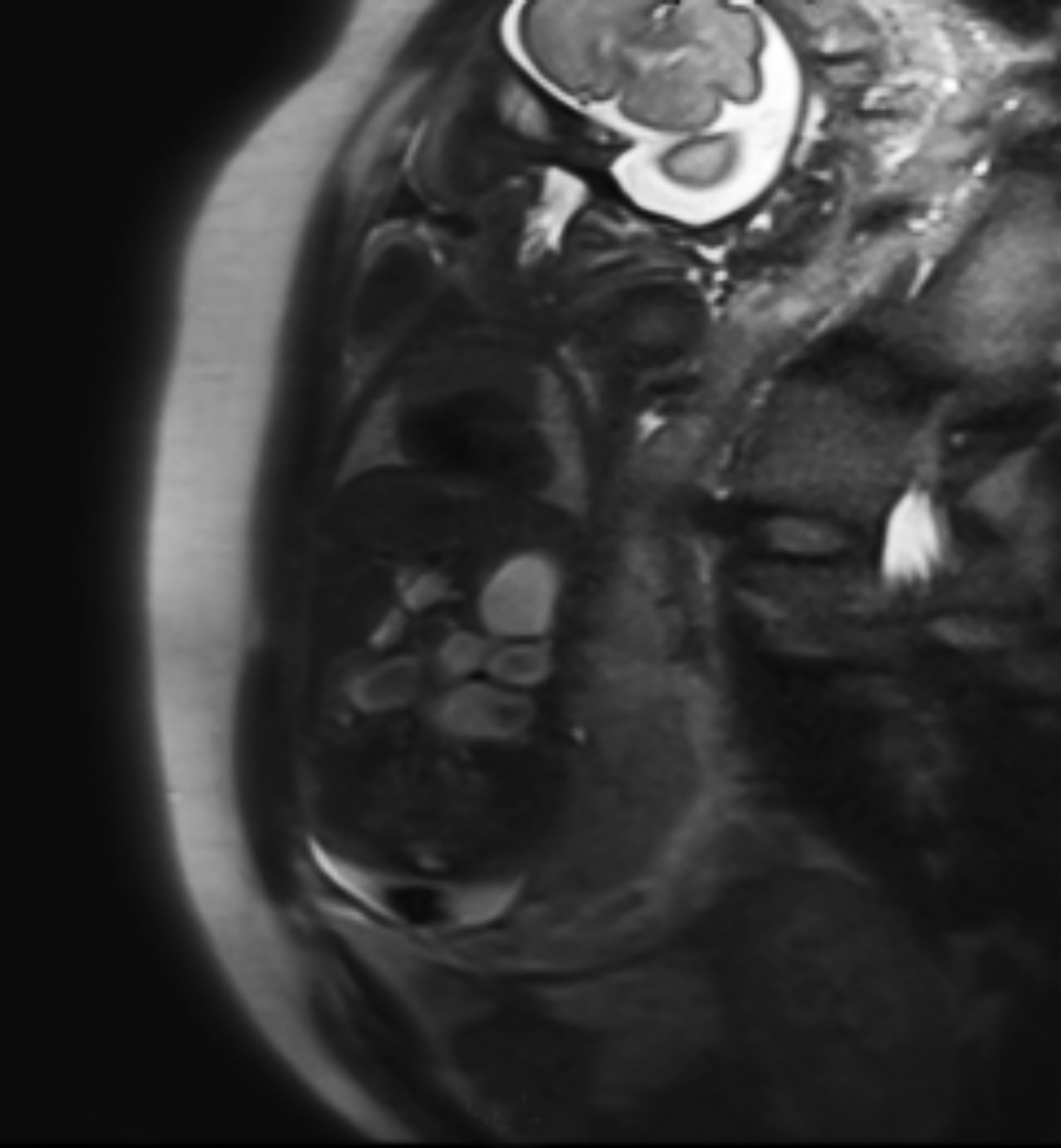
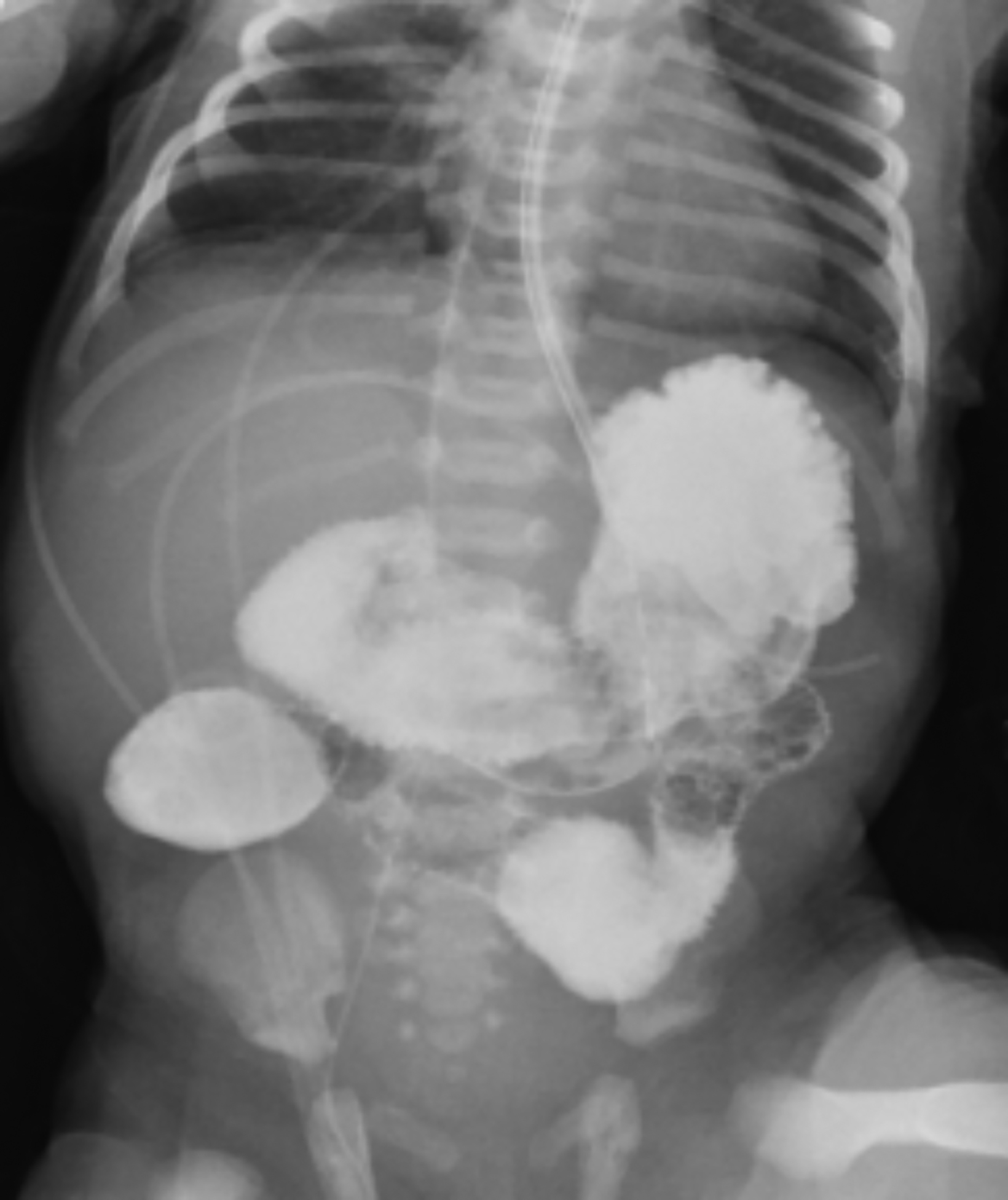
Fetal MRI performed at 28 weeks’ gestational age demonstrated multiple fluid-filled and dilated loops of bowel in the left upper abdomen with some extension into the right abdomen (Figure 1). Residual distal loops of bowel and colon were decompressed. Abdominal radiography performed shortly after birth revealed a gas-filled stomach and dilated duodenum and proximal jejunum with a suction catheter present (Figure 2).
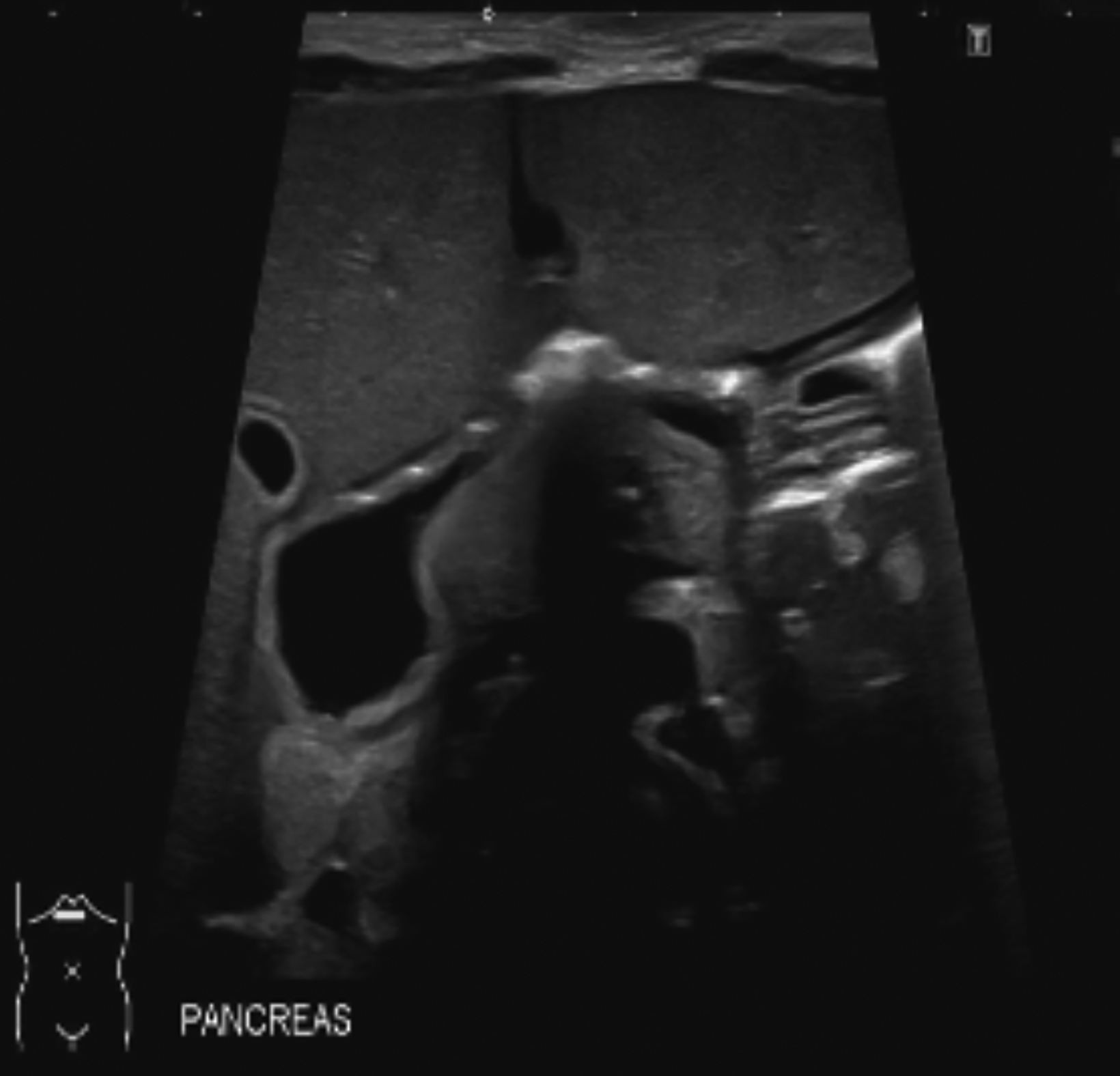
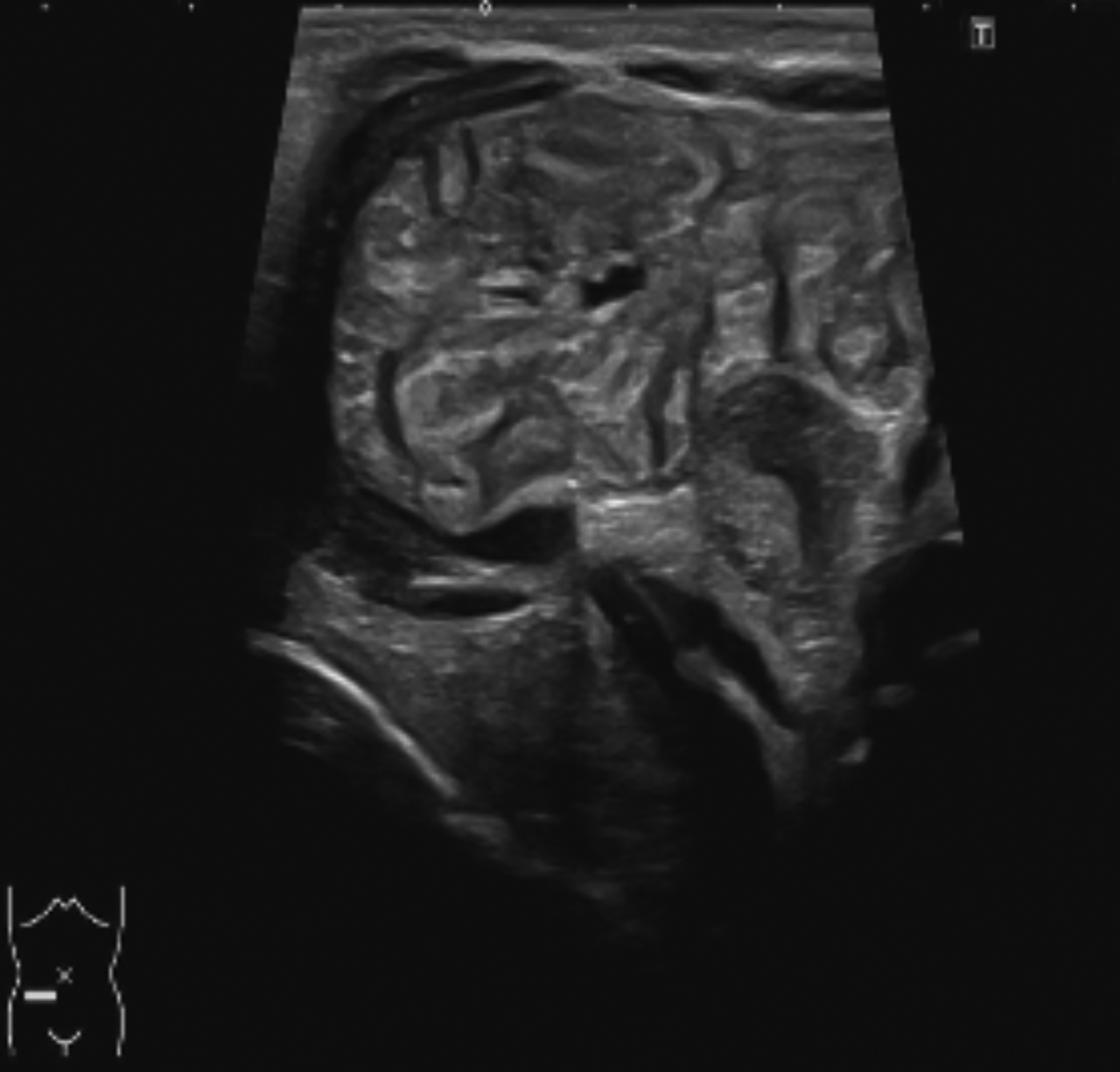
Subsequent UGI with SBFT demonstrated a distended duodenum and proximal jejunum that abruptly ended in the right abdomen, with a complete paucity of bowel gas distally (Figure 3). Delayed (100-min) abdominal radiography demonstrated the lack of contrast progression (Figure 4). Abdominal ultrasound revealed a dilated, fluid-filled duodenum and dilated loops of proximal jejunum, with the remaining abdomen appearing unremarkable (Figures 5, 6).
Subsequent exploratory laparotomy revealed a proximal jejunal atresia with two additional distal atretic segments, plus an “apple peel” deformity. The first atresia was noted to be located 12 cm distal to the ligament of Treitz.
Diagnosis
Jejunal atresia
Discussion
Atresia, considered one of the most common causes of congenital bowel obstruction, is characterized as a congenital defect that results in complete obstruction of the lumen.1 Jejunal and/or ileal atresia is present in 1 in 3,000-5,000 births and constitutes approximately 39% of all intestinal atresias.2 Jejunoileal atresia results from an ischemic insult during pregnancy; the injury can be secondary to intussusception, perforation, volvulus, intestinal strangulation via hernia, or thromboembolism. Additional factors such as maternal smoking and cocaine use have also been associated with intestinal atresia.3
Newborns typically present with feeding difficulties, bilious vomiting, distended abdomen, and absence of bowel movements.4 Although ultrasound is the imaging modality of choice for screening and preliminary identification of fetal abnormalities, MRI evaluation of the fetal gastrointestinal tract is increasingly utilized.2 Postnatally, fluoroscopic contrast studies can be helpful in assessing the location and type of obstruction prior to surgery.
Conclusion
Atresia is a common form of bowel obstruction that appears as an abrupt, rounded end to a lumen. Early diagnosis and prompt surgical intervention is key to avoiding bowel ischemia and restoring continuation of bowel.
References
- Wesson DE. Intestinal atresia. UpToDate. 2019. https://www.uptodate.com/contents/intestinal-atresia. Accessed December 2019.
- Rubio EI, Blask AR, Badillo AT, et al. Prenatal magnetic resonance and ultrasonographic findings in small-bowel obstruction: imaging clues and postnatal outcomes. Pediatr radiol. 2017; 47: 411-421.
- Morris G, Kennedy Jr. A, Cochran W. Small bowel congenital anomalies: a review and update. Curr Gastroenterol Rep. 2016; 18:16.
- Genetic and Rare Diseases Information Center (GARD). https://rarediseases.info.NIH.gov/diseases/6799/jejunal-atresia. Accessed December 17, 2019.