Rabies Encephalitis
By Qureshi PAAA
Case Summary
An adult with no known comorbidities presented to the emergency department with altered consciousness, fever, and right-sided weakness following a dog bite to the right leg 15 days prior. The patient had received two doses of anti-rabies vaccine and immunoglobulins on days 8 and 10 post-bite. On general physical examination, the patient was agitated with a positive fan test for aerophobia and hypersalivation. On neurological examination, the patient had a Glasgow coma score of 9/15. The pupils were reactive and normal in size. The cardiovascular examination and lab tests, including CBC and blood glucose, were also normal.
Imaging Findings
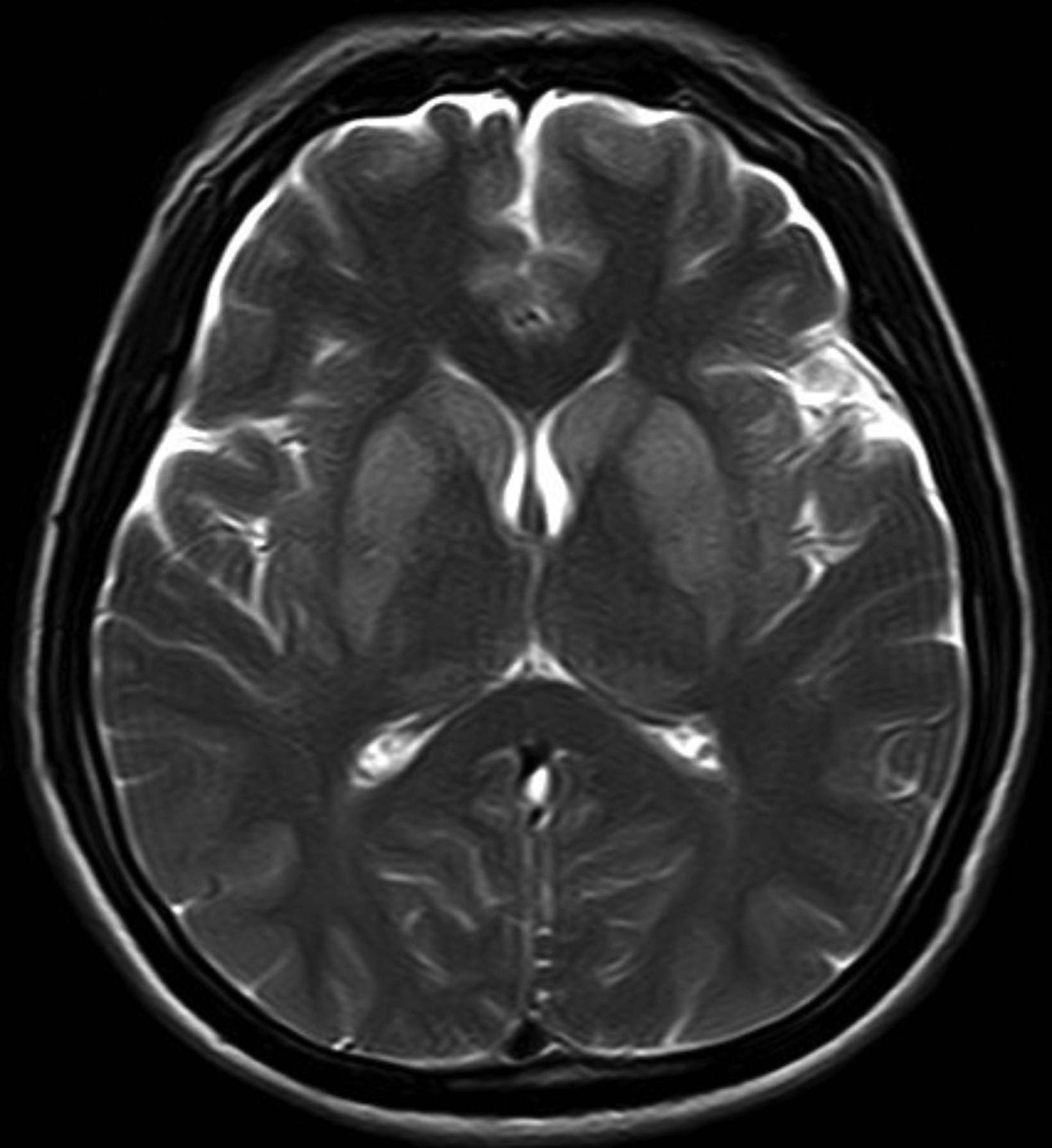
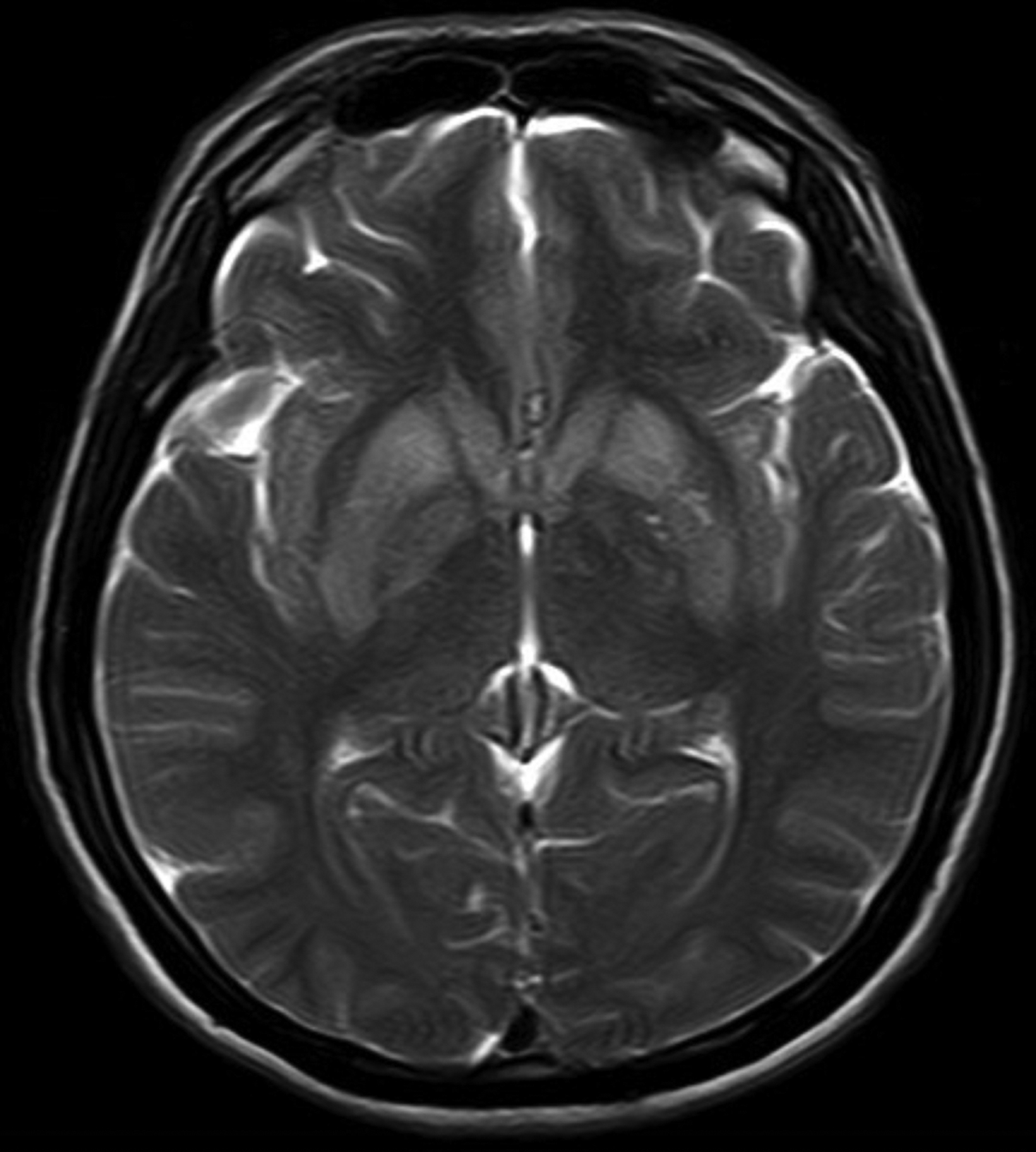
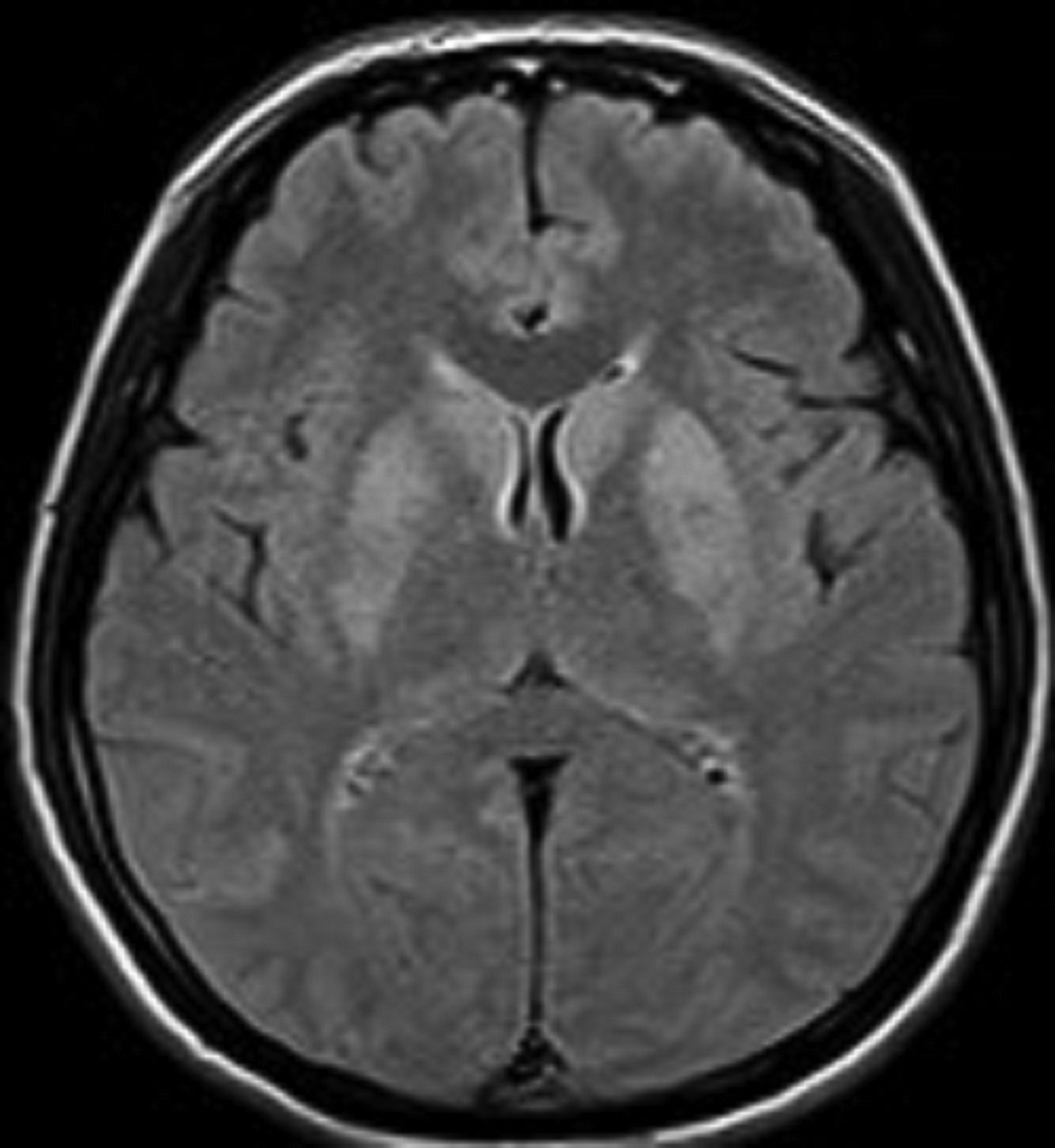
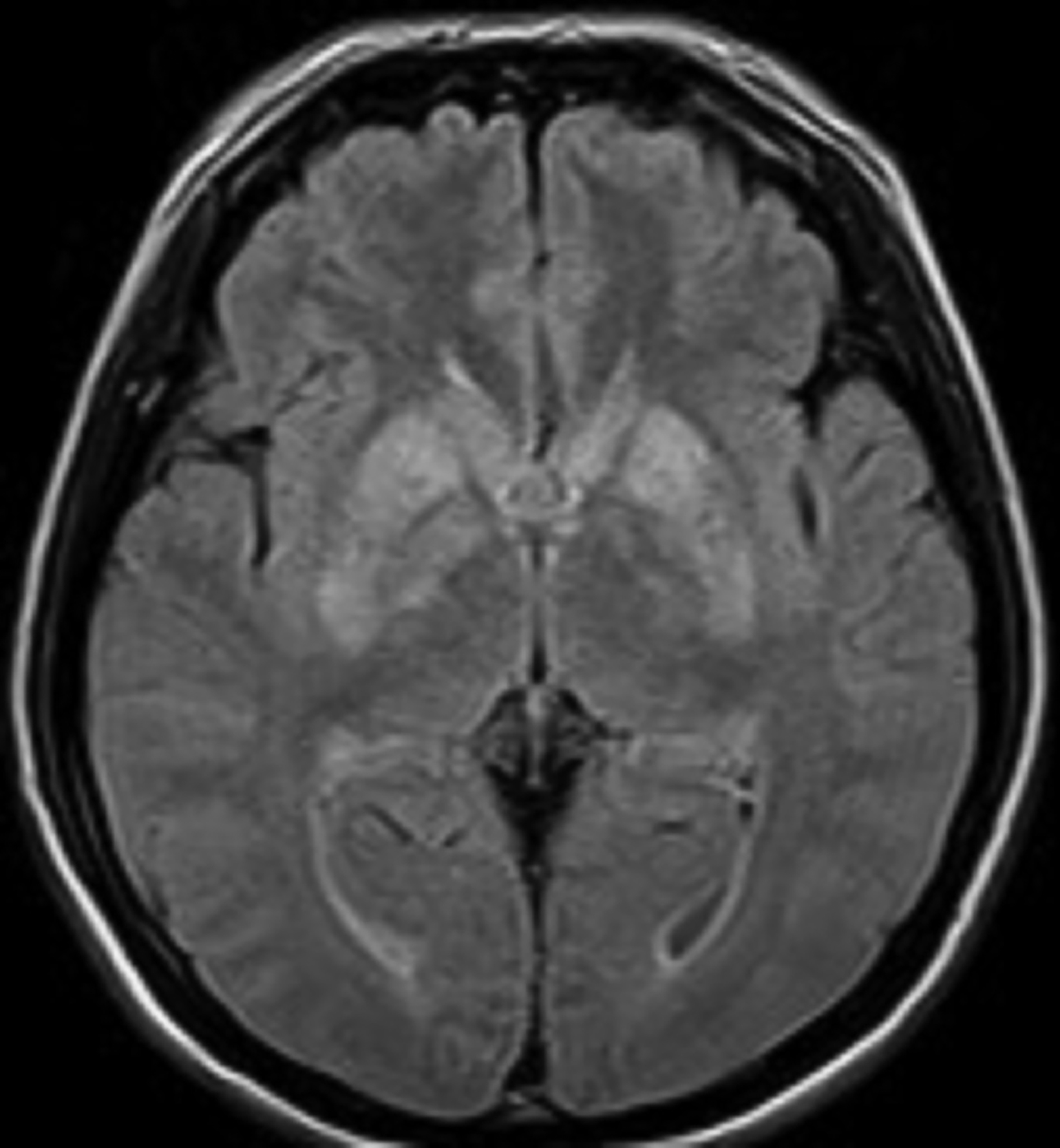
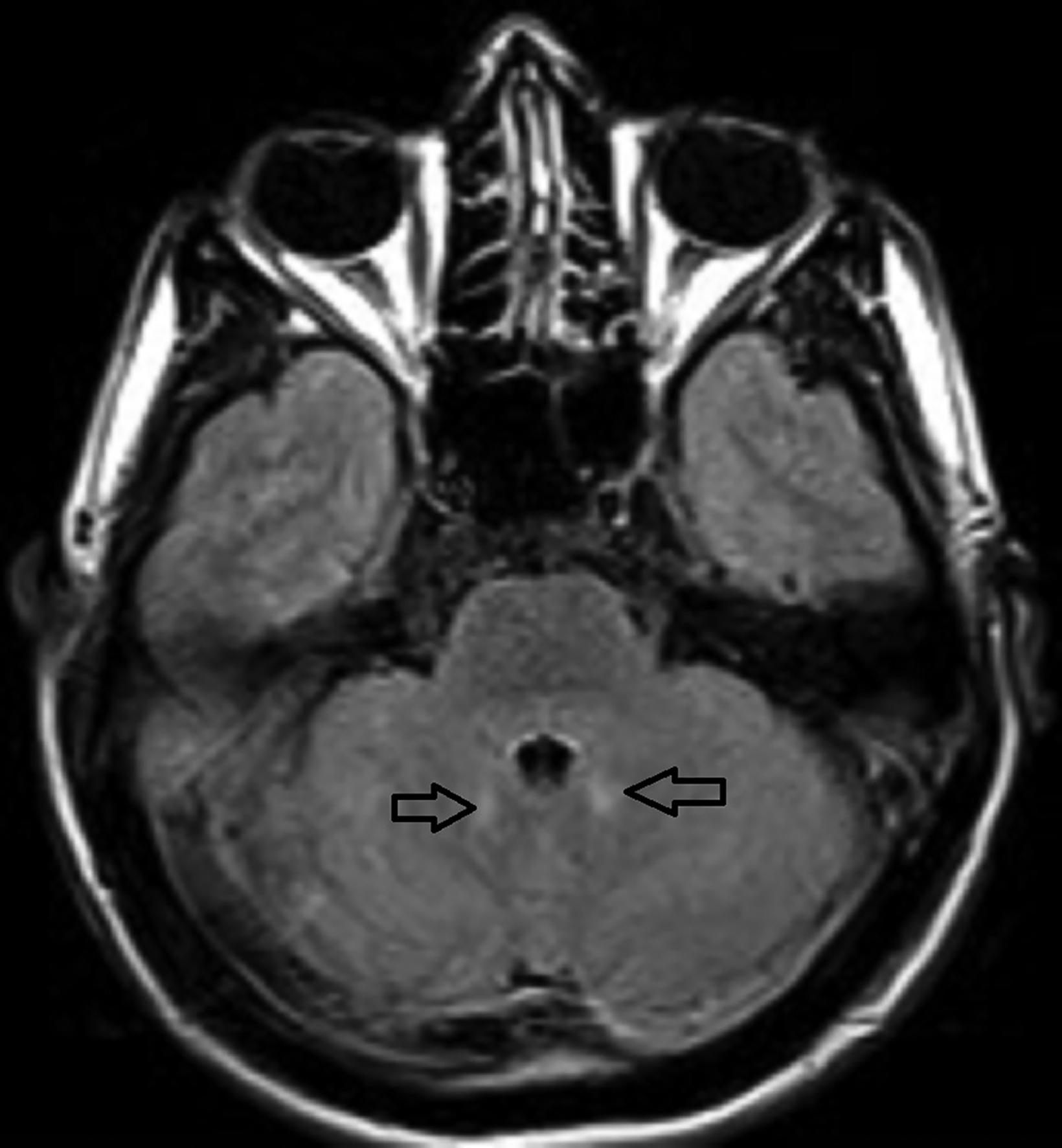
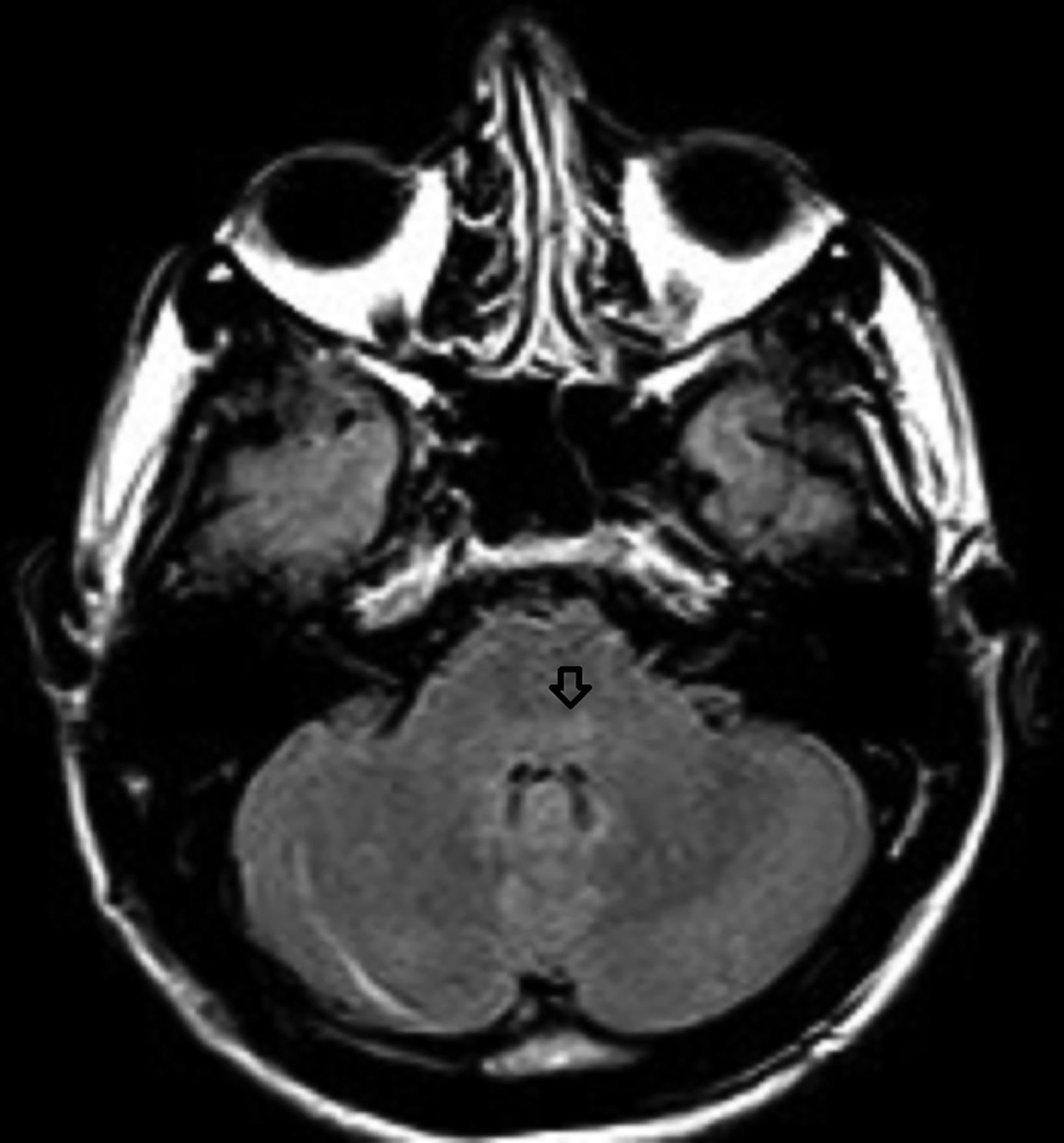
A noncontrast magnetic resonance imaging (MRI) of the brain showed bilateral symmetrical T2 and FLAIR hyperintense signal in the head of the caudate nuclei and lentiform nuclei. Additionally, symmetrical T2 hyperintense foci were seen in the bilateral dentate nuclei and dorsal pons (Figures 1,2). Neither diffusion restriction (Figure 3) nor hemorrhage were seen (Figure 4).
Diagnosis
Rabies encephalitis. The differential diagnosis includes carbon monoxide poisoning, hypoglycemia, and methanol toxicity.
Discussion
Rabies encephalitis is an acute, rapidly progressing infection of the central nervous system (CNS) caused by a virus of the Rhabdoviridae family, Lyssavirus genus. It is most frequently transmitted to humans via the bite of a rabid animal, usually a dog in developing countries and a bat in developed countries.1 Uncommon transmission routes include open wounds, aerosols, mucous membranes, and organ transplantations.2 The virus reaches the CNS through retrograde axoplasmic flow in the motor neurons from the site of inoculation and has a typical incubation period ranging from 2 to 8 weeks, depending on the viral strain.1 Furthermore, an inverse relationship exists between the viral load and proximity of the infection site to the CNS.3, 4 Clinically, there are four stages of rabies infection: incubation, prodromal, acute neurological, and coma.5
In humans, rabies presents in two clinical forms. The first is classic rabies encephalitis, which comprises 80% of cases and is equivalent to furious rabies in dogs. This form is characterized initially by nonspecific symptoms such as altered mental status, generalized malaise, inspiratory spasms, and autonomic dysfunction followed by hydrophobia, aerophobia, and hypersalivation.6
The second form is paralytic rabies, which comprises 20% of cases and is equivalent to dumb rabies in dogs. It typically is characterized by quadriparesis and bilateral facial weakness.4
MRI is the most sensitive modality for rabies; on T2 and FLAIR images it shows hyperintense signal in the brainstem, cerebellum, thalami, basal ganglia, hippocampi, hypothalami, frontal and parietal lobes, and spinal cord.7,8 No diffusion restriction or contrast enhancement is seen in the involved sites early in disease course; however, mild contrast enhancement can be seen in the brain-stem nuclei, hypothalami, spinal cord gray matter, and the intradural cervical nerve roots in comatose patients.
Petechial hemorrhage can also often be seen with disease progression, although not observed in this patient.9 There is no significant signal difference on MRI between classic and paralytic forms of rabies, but there is usually more involvement of the brain in the former and spinal cord and medulla in the latter.6 Computed tomography, which is usually not helpful diagnosing rabies, can show nonspecific hypodensities in the involved areas.10
There is no effective treatment for rabies, which is usually fatal. Pre- and postexposure vaccinations are necessary to prevent development of the disease; however, rare cases of postexposure vaccine failure have been reported.5
Some reasons for these cases given in the literature include: improper washing of bite wounds; noncompliance with the vaccination schedule; failure to administer the vaccine directly into the wound, failure to inject all wounds with, and failure to fully infiltrate the involved tissue with immunoglobulins; and delays of more than six days in administering the postexposure prophylactic vaccine.5
In our patient, the most likely cause of postexposure vaccine failure was the late presentation of the patient and subsequent late administration of the prophylactic vaccination.
Conclusion
Rabies encephalitis is fatal. Postexposure rabies prophylaxis should be administered immediately after exposure using proper technique according to WHO guidelines to reduce therapy failure.
References
- Co SJ, Mackenzie IR, Shewchuk JR. Rabies encephalitis: AIRP best cases in radiologic-pathologic correlation. Radiographics. 2015;35(1): 235-238. doi:10.1148/rg.351140035.
- Awasthi M, Parmar H, Patankar T, Castillo M. Imaging findings in rabies encephalitis. AJNR Am J Neuroradiol. 2001;22(4):677-680. https://www.ajnr.org/ content/22/4/677.
- Mrak RE, Young L. Rabies encephalitis in humans: pathology, pathogenesis and pathophysiology. J Neuropathol Exp Neurol. 1994;53(1):1-10. doi:10.1097/00005072-199401000-00001.
- Tirawatnpong S, Hemachudha T, Manutsathit S, Shuangshoti S, Phanthumchinda K, Phanuphak P. Regional distribution of rabies viral antigen in central nervous system of human encephalitic and paralytic rabies. J Neurol Sci. 1989;92(1):91-99. doi:10.1016/0022-510x(89)90178-0.
- Tinsa F, Borgi A, Jahouat I, Boussetta K. Rabies encephalitis in a child: a failure of rabies post exposure prophylaxis?. BMJ Case Rep. 2015;2015:bcr2014206191. Published 2015 Jan 14. doi:10.1136/bcr-2014-206191.
- Laothamatas J, Hemachudha T, Mitrabhakdi E, Wannakrairot P, Tulayadaechanont S. MR imaging in human rabies. AJNR Am J Neuroradiol. 2003;24(6):1102- 1109. https://www.ajnr.org/content/24/6/1102.
- Mani J, Reddy BC, Borgohain R, Sitajayalakshmi S, Sundaram C, Mohandas S. Magnetic resonance imaging in rabies. Postgrad Med J. 2003;79(932):352-354. doi:10.1136/pmj.79.932.352.
- Pleasure SJ, Fischbein NJ. Correlation of clinical and neuroimaging findings in a case of rabies encephalitis. Arch Neurol. 2000;57(12):1765-1769. doi:10.1001/ archneur.57.12.1765.
- Rao AS, Varma DR, Chalapathi Rao MV, Mohandas S. Case Report: Magnetic resonance imaging in rabies encephalitis. Indian J Radiol Imaging. 2009;19(4):301-304. doi:10.4103/0971-3026.57214.
- Sing TM, Soo MY. Imaging findings in rabies. Australas Radiol. 1996;40(3):338-341. doi:10.1111/j.1440-1673.1996.tb00415.x.
Syed Abdullah Shah Institute of Medical Sciences, Sehwan, Sindh, Pakistan