Tele-Ultrasound: Meeting Global Imaging Challenges
Images



According to The World Health Organization (WHO), diagnostic ultrasonography (US) is one of the most important technologies in developing countries. Access to US is now considered a minimal global standard. The WHO reports that medical imaging is needed for diagnosis in 20-30 percent of clinical cases, and that US and/or conventional radiology would be sufficient for up to 90 percent of those cases.1 Unfortunately, two-thirds of the world’s population, especially people living in low- and middle-income countries (LMICs), have no access to medical imaging. For example, in Malaysia, there are approximately 30 radiologists per million people compared to the desired goal of 50 per million in 2030.2
The availability of US services in underserved areas is limited by many factors. A lack of trained sonographers/sonologists and appropriate equipment, along with inadequate infrastructure, are two major ones.3 To help solve these challenges, telemedicine, including teleradiology and tele-ultrasound (TUS), can be employed to provide responses to clinical situations in the absence of on-site specialists.4 Indeed, multiple studies have shown that TUS improves access to, and reduces the costs of, healthcare in remote geographic regions with limited infrastructure.3,5
Tele-ultrasound can take place in two ways: asynchronously or in real time. In asynchronous TUS, static images or clips are captured and stored for later review by radiologists (a process also known as “store and forward”). The benefits of asynchronous TUS include training local practitioners to obtain clips of a body region or target organ using basic scanning protocols. One method consists of volume sweep imaging a target to create a tomographic series or 3D capture of the region.6 In an emergency, first responders can obtain and send a sweep to a remotely located radiologist for interpretation, if not for immediate evaluation, then for later validation/refutation of a preliminary diagnosis.
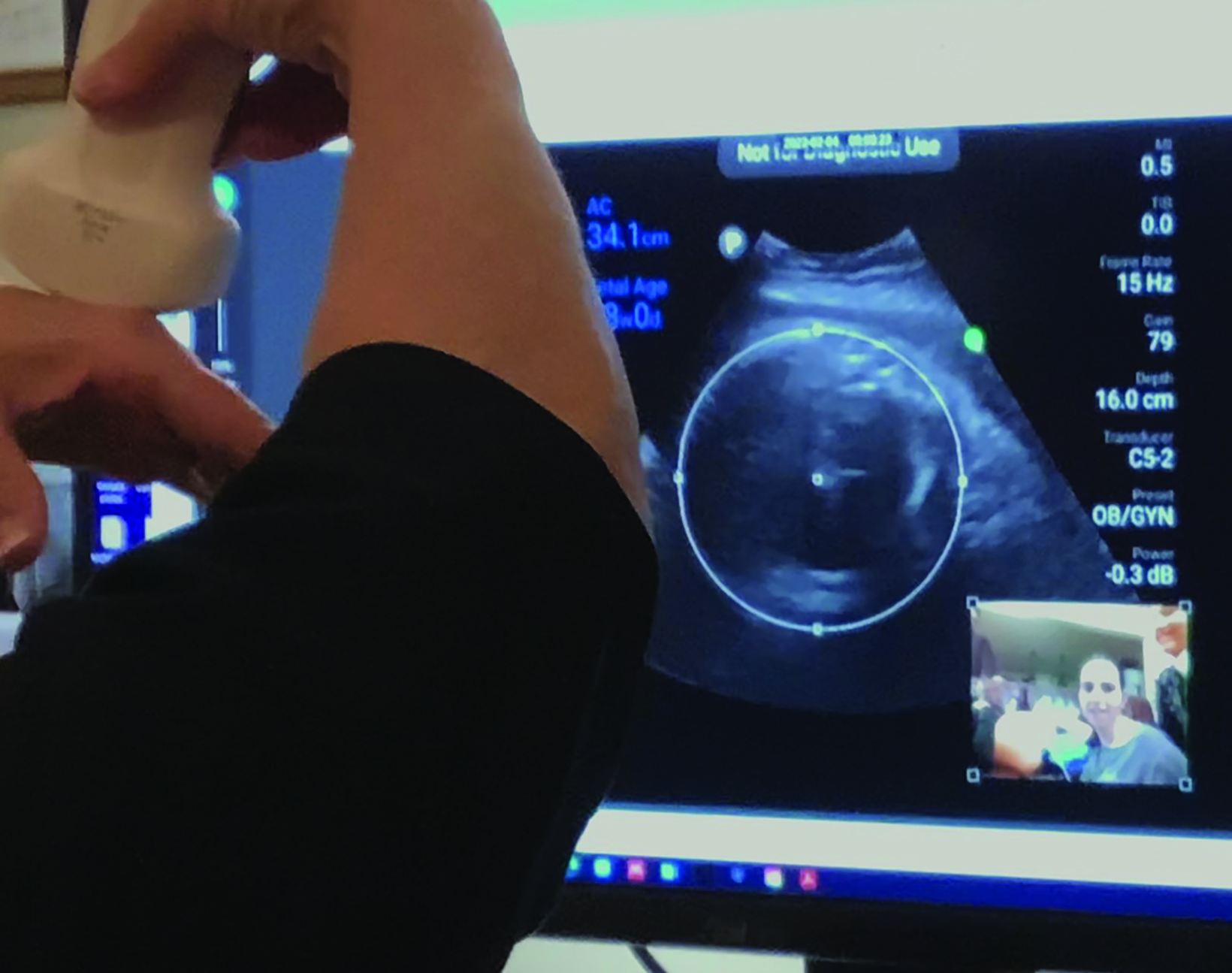
Real-time TUS, on the other hand, allows the expert observer to be virtually present during scanning, enabling direct feedback and enhancing the expert’s ability to guide the operator and improve image quality. Real-time TUS quality is improving almost by the day. A smartphone or similar device can be connected to the probe to observe the person scanning while generating a split-screen image for both participants. One side shows the practitioner performing the scan, while the other shows the image (Figure 1). The receiving expert can remotely move a cursor over the sender’s image, demonstrating correct location or orientation. The sending provider can also move a cursor in response (Figure 2). Both participants can also view each other, allowing for virtual “hands-on” instruction (Figure 3). These capabilities have been revolutionary for US education and mentoring.
Indeed, with the growing availability of commercial off-the-shelf software, high-definition images using Windows or Android configurations can now be transferred around the world in seconds over Wi-Fi and 5G networks that provide 100 times faster data transmission rates (up to 10 gigabytes per second), and capacities more than 100 times that of 4G technology.
Tele-Ultrasound Effectiveness
Over the past 10 years, numerous studies have examined the utility of TUS in settings where other technologies are unavailable, cost-prohibitive, or unable to be properly maintained.
Table 1 offers a summary of systematic reviews of TUS publications from 1950 to 2020.1
Asynchronous training with TUS suffers from difficulty in recruiting and retaining reliable learners, however it does provide for learner flexibility. Many pilot projects in LMICs have been initiated by organizations such as RAD-AID™. Asynchronous training is followed by hands-on training/mentorship. Outcomes data will be essential to validate the effectiveness of TUS as it expands throughout these regions.
Novel Approaches to Come
Telemedicine is quickly becoming adaptable to many different situations and scenarios. FaceTime™ video conferencing via iPhone, for example, is demonstrating utility not just with telemedicine in general but also in ultrasound consultation specifically.
One drone-based product involves flying US units to inaccessible locations for catastrophic emergencies, and to vulnerable populations for whom transport is impractical or undesirable. This can be particularly useful in war zones, wilderness rescues, and other areas and circumstances with little access to imaging.
In obstetric US, a novel, self-operated home system that attaches to a smartphone (known as INSTINCT®) is being used for fetal assessment, including a basic biophysical profile. In one study, it has demonstrated high accuracy in assessing fetal heart rate, amniotic fluid index, and fetal tone.7
Artificial Intelligence and Tele-Ultrasound
Amid the limited resources and lack of expert sonographers in many LMICs, artificial intelligence (AI) offers the opportunity for even the inexperienced to acquire diagnostic-quality images. In the US and Europe, some agencies have been granted regulatory approval to process images using AI guidance. In this process, after entering anthropometric information, a transducer is placed on the patient. The operator is instructed on probe placement and movement, and the picture is automatically captured as soon as the device detects a high-quality image, essentially performing volume sweep imaging. AI-assisted TUS is still investigational; to ensure accuracy, a large database of condition-specific and normal images will be required to build the algorithms needed to train the technology. Nevertheless, AI-assisted guidance for all US procedures may eventually become commonplace. Deep-learning algorithms for precision US interpretation are also in early development; these tools are being studied for their ability to evaluate condition and injury severity for real-time clinical decision making.8
Conclusion
Tele-ultrasound has been shown to improve access to, and reduce the costs of healthcare in, remote areas with limited infrastructure. Rapidly evolving technology will promote increased implementation of TUS, especially in settings with few trained professionals. Affordable pocket/hand-held devices are increasingly available globally, providing excellent platforms for the application of TUS. As global connectivity expands, particularly with improved cellular and internet access, TUS is quickly becoming more feasible worldwide.
Although TUS applications are unlikely to fully replace hands-on scanning or human professional judgment in clinical decision making, they will continue to advance in the years ahead. Radiologists must remain up to date on technical innovations and consider leveraging TUS as a tool to expand high levels of care to those in need around the world.
References
- Recker F, Höhne E, Damjanovic D, & Schäfer VS. US in Telemedicine: A Brief Overview. Applied Sciences. 2022; 12(3):958. https://doi.org/10.3390/app12030958
- Henderson M. Radiology facing a global shortage. RSNA News. May 10, 2022. https://www.rsna.org/news/2022/may/global-radiologist-shortage.
- Ewing B & Holmes D. Evaluation of current and former teleradiology systems in Africa: A review. Annals of Global Health. (2022), 8(1); 43.
- Arbeille P, Zuj K, Saccomandi A, Ruiz J, Andre E, de la Porte C et al. Teleoperated echograph and probe transducer for remote US investigation on isolated patients. Telemedicine and e-Health. 2016; 22(7); 599-607
- Britton N., Miller M, Safadi S, Siegel A, Levine A, & McCurdy et al. Tele-US in resource-limited settings: A systematic review. Frontiers in Public Health. 2019 7(244); 1-13.
- Carbone MF. A tele-ultrasonographic platform to collect specialist second opinion in less specialized hospitals. Updates in Surgery. (2018) 70; 409-413.
- Hadar E, Wolff L, Tenenbaum-Gavish K, Eisner M, Shmueli A, Barbash-Hazan S et al. Mobile self-operated home US system for remote fetal assessment dur- ing pregnancy. Telemedicine and e-Health. 2022; 28(1); 93-101.
- Liua S, Wanga, Yangb X Leia B, Liua L, Lia S, et al. Deep learning in medical ultrasound analysis: a review. Engineering. 2019; S(2); 261-275. https://doi. org/10.1016/j.eng.2018.11.020
Citation
DL D, RD H.Tele-Ultrasound: Meeting Global Imaging Challenges. Appl Radiol. 2024; (1):38-39.
January 24, 2024