Technology and Industry: GE and Amersham join forces: A conversation with Dan Peters
Images
Recently, General Electric Company (GE) completed the acquisition of life sciences/diagnostic imaging giant Amersham plc. Together, these companies will form a new division known as GE Healthcare with a focus on imaging, diagnostic pharmaceuticals, and drug discovery. Dan Peters, President of Medical Diagnostics at GE Healthcare, recently spoke with Applied Radiology about the acquisition and its impact on the future of diagnostic imaging.
Applied Radiology: How large is the new company? How will it be structured?
Dan Peters: GE Healthcare is approximately a $14 billion global business. It is a distinct unit of GE. We are going to spend approximately $2.7 billion a year in research and development. We have roughly 42,500 employees worldwide. Sir William Castell, who was the CEO of Amersham plc, is now the President and CEO of GE Healthcare. That is part of the intention to globalize the GE Healthcare business and to be a big player in Europe, as well as the rest of the world.
GE Healthcare Technology, the old GE Medical Systems, will continue to be headquartered in Waukesha, WI, and will continue to be led by Joseph Hogan, President and CEO. This will still be an $11 billion business, with products and services in areas like diagnostic imaging equipment, ultrasound, interventional equipment, and information technologies.
The other part of GE Healthcare is called GE Healthcare Bio-Sciences. Peter Loescher will be President and CEO of Bio-Sciences. It is the pharmaceutical part-the in vivo medical diagnostics business that I run, and the two other businesses: protein separation and discovery. Importantly, we are going to headquarter this business in Chalfont St. Giles, UK, a town just outside London. This, too, is a reflection of GE's ambition to participate more in the global economy, not just in the United States.
These two businesses will work together, trying to build upon each other's strengths, learning from each other, as much as possible, about how we can be stronger and contribute more to the diagnostic community. We think it gives us a good platform upon which to identify synergies for good ideas, good thinking, and best practices.
AR: What was it that brought these two companies together?
DP: Before the acquisition, GE, as it was previously defined, was the leader in its particular footprint of business with technologies, and Amersham was the leader in its particular footprint of business with biologics and pharmaceuticals. We think it makes great sense.
I think the real key, however, is that we both share a vision of the future of diagnostics, of personalized medicine, molecular diagnostics, and really doing diagnosis at the disease level and being an integral part of the provision of healthcare. We both shared that vision before we became joined, and it was that shared vision that really brought the two businesses together. We see molecular imaging, which is getting diagnosis right down to the disease level, as a very important step in the future of healthcare.
AR: Will this acquisition affect how new products are developed?
DP: Yes. When it comes to the development of products, our biological research will continue to be within Bio-Sciences, and technology will stay on the Technology side. But, absolutely, if there is an opportunity to provide better tools for the diagnostic physician so that they can do their job more effectively, then certainly we will look for ways to answer that need. It's all an issue of what can we do to help all physicians treat their patients more effectively. And to the extent that we can combine some of our thinking to help come up with solutions, we are certainly going to do that.
AR: How will this affect the day-to-day practice of the typical radiologist?
DP: We think that the diagnostic physician will be very well served by this. We firmly believe that diagnostic information will be critical in providing good healthcare in the future. We believe that good diagnosis-early diagnosis-allows either early intervention or the most effective treatment to be applied to the patient, thereby getting better results and, as much as possible, controlling the cost.
AR: Do you think this joining of forces will help bring mo-lecular imaging to the forefront of radiologic practice?
DP: Molecular imaging is still in the early stages, and we think this will help us bring it to the physicians faster wherever possible. If we have any technical hurdles along the way, hopefully, we can address them more effectively now.
That's the whole name of the game: to get molecular, personalized imaging products out to the physicians as quickly as we can with good information, good clinical data, and good protocols as to how they can be used.
AR: What do you foresee as being the most significant advancements in diagnostic imaging over the coming decade?
DP: We think that in 5 to 10 years you are going to see good personalized medicine information, good molecular imaging. I really do think that that is the direction imaging is going to go: continued advancements in equipment and, on the biological side, the evolution from anatomic information to the physiologic, biologic information. That would be a major step. I think these are major, evolutionary changes.
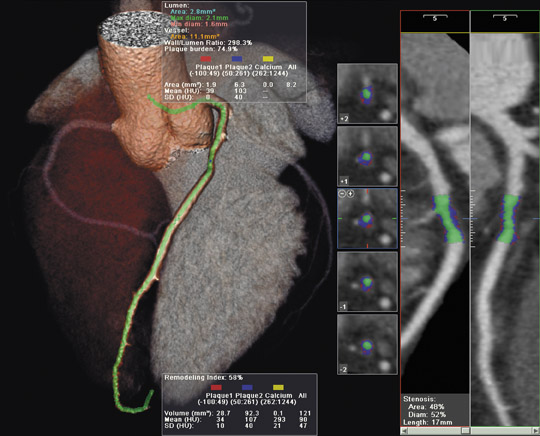
Historically, diagnostic physicians are left with seeing the results of a disease that already took place. If we can get good molecular imaging earlier, then intervention can take place earlier as well (Figure). The tremendous growth that you have seen in interventional imaging and interventional radiology will expand rapidly, and we can start diagnosing things earlier and helping patients much earlier in the disease process.
AR: Within which clinical areas will GE Healthcare be focusing their new product development?
DP: At GE, the areas that we are focusing on are cancer, heart disease, and neurological disorders. We know that approximately 1 in 3 persons will contract cancer before the end of their lifetime. We know that 50% of the patients who have heart disease die after their first heart attack. We also know that 20% of the people aged 55 to 84 suffer from Alzheimer's disease. Those are huge areas that require real investment to try to get to the disease earlier. These are areas that we think really warrant the emphasis on molecular imaging.
We have a continuum in terms of the healthcare paradigm that we like to follow whenever possible: we are trying to be able to predict, then diagnose, then inform and treat. We see that as an evolution of the diagnostic paradigm going forward for the next 5 to 10 years or beyond.
On the "predict" side, we do see that this is an area in which we are going to have a molecular understanding of disease, looking at the fingerprint of a disease, so we can tell the person if they have the potential for a particular disease. On the "diagnosis" side, we think that if you can find a disease earlier, then you can treat it earlier, and we can limit the intervention into a patient and have a better chance for effective treatment. On the "inform" side, we just think that with molecular information, you can give better care; you can give excellent patient information- when, where, and how a disease should be treated. On the "treatment" side, we want to be able to read the genes, understand the disease at a very early level, and, as I say, treat it as early as possible.
We really think that if we can detect it earlier, physicians may be able to stop disease very early in the process and really limit the morbidity of the disease.
AR: What kind of feedback have you received from radiologists regarding this acquisition?
DP: The feedback we are getting on the acquisition of Amersham has been positive. I think we are positioned to address the biggest challenges in healthcare and to create the transformation of diagnostic imaging to a new medical imaging area. We think that we are well-positioned to shape a new age in medicine.