Low dose MDCT: Iterative reconstruction technique sets new standards
Images

Presentation
A 3-day-old male premature infant with echocardiography findings of right aortic arch, suspected aberrant left subclavian artery origin from the aortic arch, and possible severe coarctation of the aorta versus aortic interruption, presented for a computed tomography angiogram (CTA) of the thorax to evaluate cardiothoracic vasculature prior to surgical repair.
Imaging Findings
CTA of the thorax was performed on a 128slice MDCT scanner, which produces 128 slices of image data (Ingenuity CT, Philips Healthcare, Cleveland, OH) with the following protocol parameters: 64 × 0.625 mm collimation, 2 mm/1 mm slice thickness/slice increment, 80 kV, 50 mAs, scan length 81 mm, CTDIvol 1.0 mGy.Via a 24 gauge IV in the left hand, 4 CC of Iopromide (Ultravist® 370, Bayer Healthcare Pharmaceuticals, Wayne, NJ) was delivered as a bolus immediately prior to initiation of the scan. Scan duration was 2.31 sec.
Calculation of estimated effective dose is accomplished by recognizing the current recommendations and standards set by the American Association of Physicists in Medicine (AAPM) Report 961 and the International Electrotechnical Commission (IEC)
International Standard 606012442, respectively. Report 96 indicates the age-appropriate conversion factor (k) is 0.039 mSv•mGy1 •cm1 for a newborn chest exam and assumes use of the 16 cm CTDI phantom. The estimated effective dose is calculated by multiplying the dose-length product (DLP, DLP = CTDIvol × irradiated z-axis length) provided on the CT scanner at the time of the scan by the age-appropriate conversion factor (k). Because the scanner reference phantom based on the current edition of IEC 60601244 is 32 cm for thoracic examinations, even for pediatric patients, but the reference used for the newborn chest conversion factor in Report 96 is a 16 cm phantom, the CTDIvol (and, hence, the DLP) must be doubled prior to calculating the estimated effective radiation dose. Therefore, the estimated effective radiation dose for this examination was 0.63 mSv (based on CTDIvol 1.0 mGy, irradiated z-axis length 8.1 cm, DLP = 8.1 mGy•cm multiplied by 2 and k 0.039).
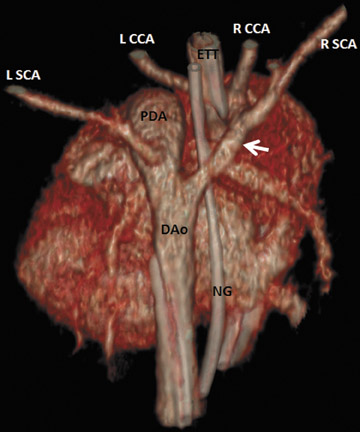
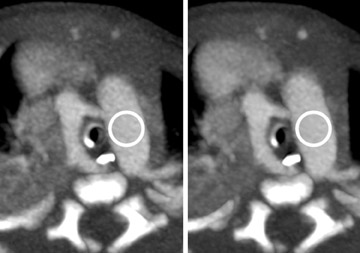
Image reconstruction and postprocessing techniques included the standard filtered back projection (FBP) images, iterative reconstruction technique (iDose4, Philips Healthcare) images, and 2-dimensional maximum intensity projection (MIP) and 3-dimensional surface rendered images of the heart and cardiothoracic vessels (Figures 1 and 2).
Diagnosis
Hypoplastic right aortic arch. Brachiocephalic artery branching: left common carotid artery, right common carotid artery, and right subclavian artery. Patent ductus arteriosus (PDA) with left subclavian artery arising from the PDA.
Discussion
CTA was chosen over magnetic resonance imaging (MRI) in this case because of the rapidity of the exam, as the patient suffered from neurologic and cardiac labiality. Aortic arch, pulmonary artery, PDA, and brachiocephalic artery anatomy were clearly depicted utilizing CTA in this patient with a very low radiation dose, 0.63 mSv. The CTA findings confirmed the echocardiographic impression of a right-sided aortic arch and PDA, and clarified the brachiocephalic artery branching, including the true order of branching from the aortic arch and that the left subclavian artery did not arise from an anomalous origin (typically from the distal aortic arch or proximal descending aorta), but rather from the PDA. This differentiation is clinically relevant in that the origin of the left subclavian artery is likely to include ductal tissue, which will certainly result in stenosis or even occlusion of the left subclavian artery origin as the ductus closes.
The right aortic arch combined with the PDA forms a true vascular ring which completely surrounds the trachea and esophagus. Right aortic arch with PDA, or ductus ligament; right aortic arch with aberrant left subclavian artery and PDA (or ductus ligament); and double aortic arch are the 3 forms of true vascular ring.3 A vascular ring is clinically important as its presence can cause extrinsic mass effect upon the trachea and esophagus, resulting in respiratory abnormalities or dysphagia. After the PDA closes, the patient may continue to be symptomatic as the ring remains complete due to the presence of the ductus ligament. Knowing that a true vascular ring is present and the branching order of the brachiocephalic arteries is crucial information to the cardiothoracic surgeon who will perform surgery on this infant to augment the hypoplastic aortic arch, release the confines of the vascular ring, and reinsert the left subclavian artery into the reconstructed aortic arch. With 3-dimensional reconstructed images of the cardiothoracic vascular structures in this case, the surgeon can confidently understand the anatomy and plan the approach to and steps in surgical repair prior to opening the patient’s thorax.
Normally, 6 paired primitive aortic arches connect anterior and posterior aortae. During embryogenesis, each arch undergoes systematic growth and regression to form the aorta, pulmonary arteries, and the brachiocephalic arteries. When there is incomplete regression or failure of persistence of a segment of one of the primitive arches, congenital anomalies of the aortic arch result. When the left fourth arch (which usually persists as a left aortic arch) regresses, and the right fourth arch persists, there is a right aortic arch.The left sixth arch normally becomes the left pulmonary artery and the ductus arteriosus, and the dorsal aorta becomes the descending thoracic aorta.3 These are the structures seen in the patient presented in this case report.
The Ingenuity CT is a 128-slice MDCT scanner capable of real-time processing of image data using an iterative reconstruction technique (iDose4), which is emerging as an important method for reducing quantum mottle in noisy data sets and for allowing lower radiation dose examinations, while maintaining image quality. In this patient, the scan was performed using an approximate 40% reduction of radiation dose by lowering the mAs to 50. By reducing the radiation dose by 40%, image noise is increased by 23%, according to the equation for the established inverse square relationship between dose and quantum noise; %NR = 100 × (1√100% DR/100). Using iDose4, image noise is reduced from standard deviation of Hounsfield unit (HU) measurement of 21.6 in the FBP image to 14.3 in the iDose4 image, a reduction of 34%, and net decrease in noise of 11% (Figure 3). Anecdotally, due to reduced noise, iDose4 image data postprocessing is more efficient and the diagnostic quality of the images is increased.
Conclusion
Cardiothoracic CTA is a useful examination for diagnosis of congenital heart disease and is a reasonable examination to perform, especially when the radiation dose follows the ALARA concept. CT data processing using iDose4 reduces image noise and allows substantially decreased radiation doses, providing radiologists with the tools to set new standards in the meaning of reducing radiation dose.
References
- American Association of Physicists in Medicine. The measurement, reporting, and management of radiation dose in CT: report of AAPM Task Group 23 of the Diagnostic Imaging Council CT Committee. College Park, MD: AAPM, 2008: AAPM report 96.
- International Electrotechnical Commission. Medical electrical equipment, part 244. Particular requirements for the safety of Xray equipment for computed tomography. Geneva, Switzerland: IEC, September 2002: publication no. 60601244, Amendment 1.
- Shah RK, Mora BN, Bacha E, et al. The presentation and management of vascular rings: An otolaryngology perspective. Int J Pediatr Otorhinolaryng. 2007;71:5762.