Hemorrhagic Synovial Cyst
Case Summary
An adult presented with a 10-day history of lower back pain following an episode of heavy lifting. Physical examination demonstrated pain radiating down the posterior left leg, accompanied by paresthesia in the medial thigh. This pain significantly affected the patient’s mobility, but there was no bowel or bladder incontinence. Laboratory tests showed a supra-therapeutic international normalized ratio (INR) value of 4.03 due to coumadin treatment for a mechanical heart valve.
Imaging Findings
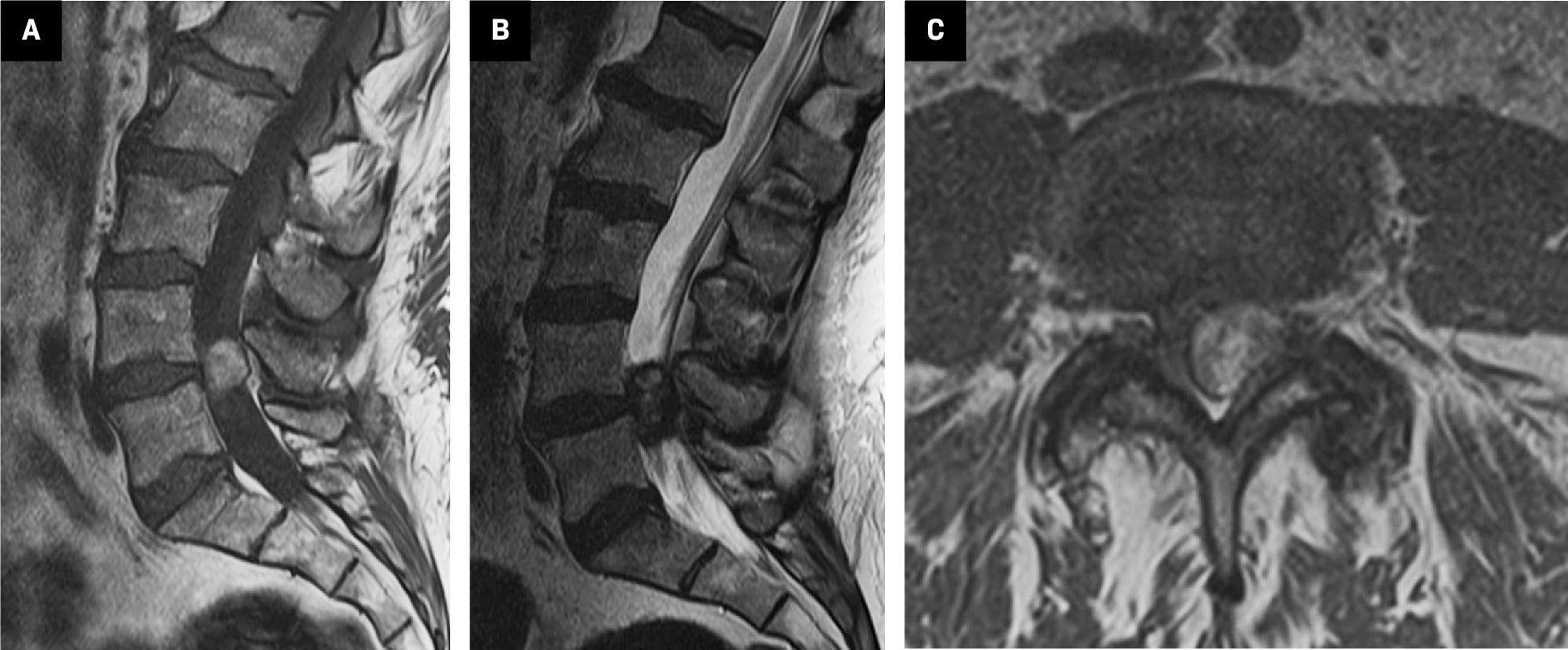
Lumbar spine MRI identified a 2.8 cm cyst with a hemorrhagic component at L4-L5, causing severe lumbar stenosis. Sagittal T1 ( Figure 1 ) demonstrated hyperintense T1 signal, suggesting hemorrhagic or proteinaceous components. Sagittal T2 MRI revealed hypointense T2 signal. Axial imaging confirmed the hyperintense T1 signal and showed the lesion projecting medially from the left L4-L5 facet joint into the left dorsolateral epidural space.
MRI of lumbar spine without contrast. (A) Sagittal T1 image demonstrates the hyperintense T1 signal epidural mass at L4-L5. (B) Sagittal T2 image demonstrates the hypointense T2 signal epidural mass at L4-L5. (C) Axial T1 image demonstrates the hyperintense T1 signal mass projecting medially from the left facet joint in the left dorsolateral epidural space.
Diagnosis
Hemorrhagic synovial cyst
Discussion
Synovial cysts are fluid-filled sacs that arise from a joint or tendon, often resulting from degenerative changes. When these cysts occur in the spine, they are typically associated with the facet joints. According to one retrospective cohort study, synovial facet cysts are found in approximately 6.5% of patients undergoing lumbar MRI.1 Hemorrhagic synovial cysts are less common, reflecting only 10% of all synovial cysts.2 Hemorrhagic cysts may be more clinically challenging owing to their often more acute symptomatology and association with more chronic degenerative spinal conditions.3
Spinal synovial cysts are encountered primarily in older individuals or in those with underlying spinal conditions such as spondylosis and spinal instability, which can result from degenerative changes or trauma. Clinically, patients typically present with lower back pain and lower extremity radiculopathy, which can be bilateral. This may sometimes lead to severe episodes resembling cauda equina syndrome.3 High-impact activities and certain sports such as tennis are linked to higher occurrence rates in younger populations, suggesting repetitive stress as a risk factor.4 Additionally, hemorrhagic synovial cysts can arise secondary to anticoagulation therapy, underscoring an iatrogenic risk factor that is relevant to this case, in which the patient had a supra-therapeutic INR.5
A retrospective study of 303 lumbar MRI scans of patients referred for back pain and radiculopathy found posterior synovial cysts to be more common than anterior cysts, with a prevalence of 7.3% and 2.3%, respectively.6 Both types are associated with facet joint osteoarthritis and may be linked to degenerative spondylolisthesis, although no direct relationship with disc disease has been found. Anterior cysts can contribute to spinal stenosis and present with symptoms such as neurogenic claudication, whereas posterior cysts, located outside the canal, may be associated with back pain and radiculopathy but are less likely to cause claudication.7
As seen in this case, synovial cysts manifest predominantly at the L4-L5 level, corresponding to this level’s biomechanical stresses and load-bearing function.2 MRI is the diagnostic modality of choice. Nonhemorrhagic cysts are typically T1 hypointense and T2 hyperintense. Hemorrhagic cysts are usually T1 hyperintense while T2 images may show varying intensities depending on protein content and age of hemorrhage within the cyst.2, 3
Treatment generally consists of surgical removal, particularly when conservative treatments fail or when cysts cause significant neurological signs or symptoms. Specifically, cyst resection via laminectomy is a safe and effective management strategy for symptomatic relief. A retrospective analysis of 194 cases showed that fusion was rarely needed post-cyst resection. The postsurgical prognosis was very good, with 91% of patients reporting good pain relief and 82% showing improvement in motor deficits.8 A recent study discussed the efficacy of facet synovial cyst rupture under CT guidance, with the best success rates involving indirect percutaneous cyst rupture (IPCR) combined with direct fenestration in cases of IPCR failure.9
Conclusion
Presenting most commonly at the L4-L5 level, hemorrhagic synovial cysts of the lumbar spine pose a distinct clinical challenge. Radiological imaging plays a pivotal role in diagnosis, and surgery remains the primary treatment strategy. Prognosis depends largely on individual patient characteristics and the presence of underlying spinal conditions.
References
Citation
PS C, JR B, S R, KC B.Hemorrhagic Synovial Cyst. Appl Radiol. 2025; (2):40-41.
doi:10.37549/AR-D-25-00073
April 17, 2025