Cardiac CT for coronary artery atherosclerosis detection: Potential applications in symptomatic and asymptomatic individuals
Images




Dr. Todoran is currently a Fellow in Cardiovascular Disease in the Division of Cardiology at Washington University School of Medicine in St. Louis, MO. In 2001, he received his MD from Indiana University School of Medicine, Indianapolis, IN. At Duke University, Durham, NC, he completed his Internal Medicine Residency in 2004 and his Cardiovascular Magnetic Resonance Imaging Fellowship in 2005. Dr. Todoran has received the American Society of Nuclear Cardiology Imaging Award and currently has research support from American Society of Nuclear Cardiology Research Foundation. In 2008, Dr. Todoran will begin interventional training at Brigham and Women's Hospital, Harvard Medical School, Boston, MA .
Despite current methods of identifying patients with coronary artery atherosclerosis, many individuals suffer cardiovascular events in the absence of established risk factors. Thus, current diagnostic paradigms for the detection of coronary artery atherosclerosis are inadequate. Consequently, there is an impetus to develop improved noninvasive imaging modalities to better detect coronary artery disease (CAD) and determine the prognosis of future cardiovascular events. Cardiac computed tomography (CT) has the capacity to directly visualize the coronary arteries. Cardiac CT can be performed to detect coronary artery stenoses and assess nonobstructive stages of coronary atherosclerosis either through calcium measurement or the analysis of calcified and noncalcified plaque. There are some clinical recommendations for the use of coronary CT angiography (CTA) for symptomatic patients, as well as for the use of coronary artery calcium (CAC) measurement in patients who are asymptomatic but are at intermediate risk for CAD events based on the Framingham risk assessment. There are currently no clinical indications for coronary CTA in asymptomatic individuals for stenosis detection or assessment of coronary artery plaque.
Coronary artery atherosclerosis is approaching epidemic proportions in the United States and worldwide. Based on data from the Framingham Heart Study, a person's lifetime risk of developing symptomatic coronary artery disease (CAD) after the age of 40 is 49% in men and 32% in women. Each year, approximately 1.8 million Americans will experience an acute myocardial infarction (AMI), or sudden cardiac death will be their first clinical manifestation of CAD. 1 Finally, despite scientific advances in diagnosis and treatment, CAD is the leading cause of death in the United States, accounting for 1 in 5 deaths in men and women. 1
Current diagnostic paradigms are failing to adequately identify asymptomatic individuals with subclincal CAD. Additionally, the work-up of symptomatic individuals is frequently cumbersome, requiring multiple tests. Consequently, a need exists for better diagnostic paradigms for the detection of CAD. One way the current approach can be improved is by the use of noninvasive imaging modalities that, ideally, can be applied to both asymptomatic and symptomatic persons. There are two issues, however. First, subclinical atherosclerosis must be detected among asymptomatic individuals earlier for the purpose of risk stratification. Second, the approach needs to identify symptomatic individuals with CAD efficiently, and more importantly, identify those with flow-limiting disease in whom the treatment paradigms differ from those with non- flow-limiting disease.
With the exception of cardiac CT, no single noninvasive imaging technology currently detects both subclinical atherosclerosis and flow-limiting CAD. As such, cardiac CT coronary artery calcium (CAC) detection and coronary CT angiography (CTA) are well positioned to identify these 2 groups of individuals.
Evolution of cardiac CT
Imaging the coronary arteries is difficult because of their small diameters and the motion during the cardiac cycle. Visualizing the lumen of coronary arteries using contrast-enhanced CTA requires maximal temporal and spatial resolution. There has been rapid advancement in cardiac CT technology. In particular, greater X-ray tube currents, faster gantry rotation times, and decreasing collimation size while increasing detector length have resulted in significant improvement of image quality. The advent of 4-slice multidetector CT (MDCT) in 2000, 16-slice in 2002, and, more recently, 64-slice has allowed for progressively higher accuracy for the detection of coronary artery stenoses. 2
Greater X-ray tube currents allow for thinner collimation and thinner slice reconstruction, resulting in improved spatial resolution. Faster gantry rotation time, as high as 330 msec for dual-source CT (DSCT), has resulted in an improved temporal resolution of 83 msec. Finally, a higher number of detector rows have led to shorter overall acquisition time, as short as 5 to 8 seconds with 64-slice CT and 1.5 sec with 256slice CT. These shorter acquisition times also make it possible to obtain images with a smaller volume of contrast. All of these advancements have led to significantly improved resolution and the reduction of image artifacts.
CAC detection of subclinical coronary artery atherosclerosis in asymptomatic individuals
Background
Little data and no current recommendations exist regarding the use of coronary CTA in the assessment of occult CAD. Therefore, this section will focus on CAC detection.
The presence of calcium in the coronary arteries occurs almost exclusively in the context of atherosclerotic changes. Thus, CAC has become a surrogate marker for coronary artery atherosclerotic plaque. 3 Detection of latent CAD in asymptomatic individuals is important since many individuals suffer cardiovascular events in the absence of established risk factors. 1 Cardiac CT can accurately detect and quantify CAC, allowing for noninvasive assessment of subclinical coronary artery atherosclerosis. As a result, CAC measurement has been proposed as a way to improve risk assessment compared with the use of traditional risk factors.
Diagnostic accuracy of CAC measurement in asymptomatic individuals
The presence of CAC is highly specific for coronary artery atherosclerosis but does not allow for determining the level of stenosis since both flow-limiting and non-flow-limiting lesions have calcification present within the intima. 4
CAC and prognosis in asymptomatic individuals
Coronary artery calcium increases with age 5 and differs based on gender and race. 6-10 Additionally, age- and gender-adjusted CAC scores have been shown to be more predictive of cardiovascular events than an absolute CAC score. 11 Several studies have found that CAC scoring provides prognostic information either alone or in combination with traditional risk factors. A recent metaanalysis reported a summary relative risk ratio of 4:3 for any measurable CAC, suggesting that a person with measurable CAC is 4 times more likely to have a cardiovascular event than an individual with a CAC score of 0. 12 Furthermore, studies have shown an incremental relationship where higher CAC scores are associated with higher relative risk ratios for cardiovascular events, and more recently, independent prediction of outcomes beyond traditional risk factors or Framingham Risk Score (FRS). 13-20 Additionally, CAC scoring has been shown to predict all-cause mortality more accurately than risk factors alone. A recent large observational study that evaluated long-term prognosis reported an age- and risk-factor-adjusted 10year survival of 99% for a CAC score of 0 compared with 89% for a CAC score >1000. 21 Table 1 summarizes recent published prognostic studies based on CAC scoring.
Diagnostic impact of CAC in asymptomatic individuals
The current guidelines in primary prevention of cardiovascular events recommend initial assessment and risk stratification based on traditional risk factors. Validated analysis from the Framingham Heart Study provides algorithms projecting the 10-year risk of having a cardiovascular event. In an effort to better identify patients at risk, governing bodies such as the American Heart Association (AHA) have proposed prevention paradigms that include diagnostic tests for atherosclerosis, such as CAC measurement. For example, the Executive Summary of Screening for Heart Attack Prevention and Education (SHAPE) Task Force 22 and the recent Guidelines for Cardiovascular Prevention in Women: 2007 Update 23 recommend further risk stratification of individuals based on the results of CAC measurement by cardiac CT in addition to their FRS. Patients with a CAC score of 0 and no risk factors are at "very low" risk, while a CAC score of 0 in the presence of traditional risk factors places a patient in the "moderate" risk category. Those who test positive for coronary artery atherosclerosis are further stratified into groups of "moderately high," ''high," and "very high" risk. 22,23
Therapeutic impact of CAC in asymptomatic individuals
Based on recommendations from multiple guidelines, individuals identified to be at risk either by FRS or the presence of subclinical coronary artery atherosclerosis are treated with goal-directed lipid-lowering therapy based on recommendations from the National Cholesterol Education Program. 24 Observational studies have shown that CAC progression is the strongest predictor of future cardiac events. 25 Small observational studies have shown that lowering low-density lipoprotein cholesterol with statins also results in the reduction of CAC. 26,27 However, the St. Francis Heart Study, comparing atorvastatin to placebo in otherwise healthy asymptomatic men and women with a CAC score above the 80th percentile for their age and gender did not confirm these findings and was unable to show a statistically different reduction in events or mortality between the 2 groups. 18
Applications of cardiac CT in symptomatic patients
Background
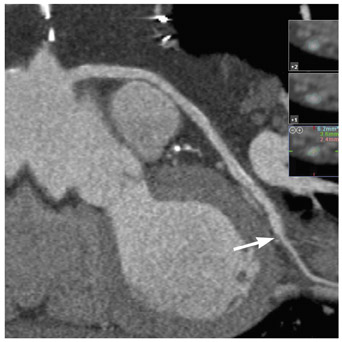
Although the presence of CAC is synonymous with coronary artery atherosclerosis, it does not imply stenosis. The disease process begins decades prior to causing obstruction of blood flow and symptoms. This is best explained by positive remodeling, where in its early stages, plaque accumulation produces a compensatory outward expansion while maintaining a constant luminal diameter. 28 Currently, invasive coronary angiography (ICA) is the reference standard for the detection of coronary artery atherosclerosis in patients with known or suspected CAD. Nearly 4 million ICA procedures are performed annually in the United States for the purpose of detecting CAD. 29 The procedure-related major complication rate for death, AMI, and stroke is <1%. 30 Because of the small but nonnegligible risk of morbidity and mortality, there has been an impetus to develop a noninvasive modality of coronary artery imaging. Furthermore, ICA is limited by its inability to see beyond the vessel lumen. In contrast, coronary CTA allows for the assessment of both luminal stenoses and identification of the extent of the plaque burden through the visualization of the vessel wall (Figure 1).
Diagnostic accuracy of coronary CTA in stable angina
Native coronary arteries- Numerous studies have compared the diagnostic accuracy of detecting coronary artery stenosis by MDCT to ICA. The diagnostic performance of MDCT varies depending on the type of analysis performed-per-segment versus the more clinically relevant per-patient analysis. Many of the early studies performed a per-segment analysis and excluded uninterpretable segments, leading to overestimation of sensitivity and specificity. Comparison of pooled per-segment accuracy with per-patient accuracy reveals an increased sensitivity from 81% to 96% at the expense of a reduced specificity from 93% to 74%. 31 There has been an overall decrease in the number of uninterpretable segments with recent technological advances; however, this still remains a problem. The diagnostic accuracy of MDCT has improved dramatically when moving from 4- to 64-slice MDCT with sensitivities and specificities in interpretable segments approaching 100% in the latter. 2 Figure 2 shows an example of a patient with flow-limiting CAD seen on coronary CTA and confirmed by ICA. Table 2 shows the diagnostic accuracy for the detection of coronary artery stenosis using 64-slice MDCT angiography compared with ICA from recent published studies.
Postrevascularization- In 2004, an estimated 1,471,000 inpatient diagnostic cardiac catheterizations were performed, with roughly 427,000 referred for coronary artery bypass graft (CABG) surgery and 1,285,000 for angioplasty. 1 Patency of bypass grafts and coronary artery stents is limited, thus follow-up examinations are inevitable.
Coronary artery bypass grafts- The development of 16-slice MDCT allowed for excellent accuracy for graft patency with sensitivities and specificities between 95% and 100%, but the accuracy for detection of graft stenosis remains suboptimal, owing to the inability to detect stenosis in the distal graft anastomosis. A recent meta-analysis compared the accuracy of distinguishing between graft occlusion and graft stenosis with 16-slice MDCT or ICA. The authors found that the number of adequately visualized vessels were much lower in the graft stenosis group compared with the graft occlusion group, 88% and 96%, respectively. 32 When compared with previous-generation scanners, recent studies using 64-slice MDCT have shown superior accuracy and higher evaluability rates of both native coronary arteries and bypass grafts, with reported sensitivities and specificities of 97%. 33,34
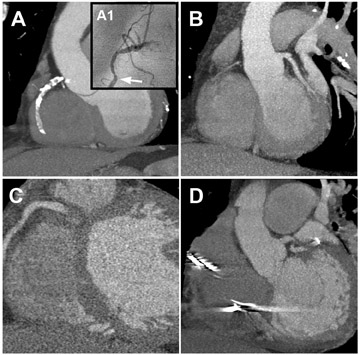
Much of the improved accuracy of imaging grafts is due to their larger diameter, minimal calcification, and reduced motion. However, for MDCT to play a significant role in the evaluation of the symptomatic post-CABG patient, a complete angiographic assessment of grafts, nongrafted arteries, and distal runoff arteries is required (Figure 3). This can prove to be a challenge in cases of advanced atherosclerosis with heavily calcified, diffusely diseased vessels.
A limited number of studies have examined the diagnostic accuracy of coexisting native CAD. First reports using 16-slice MDCT showed sensitivities and specificities of 83% and 59% with all segments compared with 100% and 93% with grafts only. 35 Recently, 2 small studies used 64-slice MDCT to evaluate bypass grafts, native (nongrafted) arteries, and distal runoff coronary arteries. The accuracy for detecting graft stenosis was similar to previous reports, but the reported accuracy for native and distal runoff coronary arteries was much worse, with sensitivities and specificities as low as 86% and 76%, respectively. 36,37 Table 3 summarizes the diagnostic accuracy in the detection of stenosis in bypass grafts versus native and distal runoff coronary arteries. The inability to adequately assess native coronary arteries severely limits the clinical utility of coronary CTA in patients after CABG surgery.
Coronary artery stents- Prior to the development of 64-slice MDCT, CT scanners lacked sufficient spatial and temporal resolution to adequately detect in-stent restenosis with reported sensitivities and specificities of 78% and 73%, respectively, using 16-slice MDCT. 38 Improved image quality with newer-generation scanners has permitted better visualization of the lumen within the coronary artery stent, as shown in Figure 4, resulting in an overall reduction in the number of uninterpretable segments from 32% to 7%. 39-41 A recent study using 64-slice MDCT reported a sensitivity of 95%, specificity of 93%, positive predictive value (PPV) of 63%, and a negative predictive value (NPV) of 99%. 41 Table 4 shows the diagnostic accuracy of MDCT angiography in the detection of in-stent stenosis from recent published studies. Factors that influence the evaluation of in-stent restenosis include stent diameter, strut thickness, and stent material. 38,42,43 Stents <3 mm in diameter with thick struts are the most challenging to evaluate. 40
Acute chest pain- Chest pain accounts for nearly 6 million visits to U.S. emergency departments annually; >50% of patients admitted to the hospital are admitted for noncardiac causes. This results in an enormous economic burden on the healthcare system. Despite conservative approaches, 2% to 10% of cases of acute coronary syndrome (ACS) are misdiagnosed. 44 As a result, there is a movement to efficiently triage patients presenting to the emergency department with chest pain to avoid unnecessary hospital admission while delivering appropriate care to patients with ACS.
Diagnostic accuracy of coronary CTA in the setting of acute chest pain
Multiple observational studies have shown that MDCT is highly accurate in detecting coronary artery stenosis and in predicting ACS in low-to-intermediate risk and high-risk patients presenting to the emergency department with chest pain. 45-48 A small randomized trial comparing MDCT to the standard of care in low-risk patients found that MDCT effectively triaged >75% of the patients either to discharge (68%) or to undergo ICA (8%). 49 Additionally, MDCT has been shown to have similar accuracy to nuclear stress testing in this setting. 45 One advantage of using cardiac CTA over stress imaging in the emergency department is that cardiac CTA can exclude extracardiac causes of chest pain, such as pulmonary embolus or aortic dissection.
Prognostic implications of cardiac CT in symptomatic individuals
Annual cardiac event rates in patients with a CAC score of 0 are extremely low. In contrast, patients with an age- and gender-adjusted CAC score >400 had annualized event rates of 13.9% for future cardiovascular events compared with 0.6% in patients with a CAC score of 0. 50 In individuals being evaluated for acute chest pain, outcome data from a few small studies with follow-up ranging from 30 days to 15 months reported no deaths or myocardial infarctions in any of the patients who were discharged directly from the emergency department with normal coronary CTA. 45,46,49 One study reported a late major adverse cardiovascular event (MACE) rate of 2.8%. From this, the authors calculated a sensitivity of 92%, specificity of 76%, PPV of 52%, and NPV of 97% for MDCT performed in the acute setting to predict overall risk of MACE. 48
One small outcome study of individuals with stable angina with a mean follow-up of 16 months has been published. Patients with a normal coronary CTA had a 1-year event rate of 0% compared with 30% in patients with any evidence of CAD on coronary CTA. Additionally, patients with flow-limiting CAD had an event rate of 63% compared with 8% in those with non-flow-limiting CAD. 51 This study further illustrates the importance of not only detecting CAD but also differentiating between flow-limiting and non-flow-limiting disease.
Diagnostic and therapeutic impact of cardiac CT in symptomatic individuals
The use of coronary CTA in low-to-intermediate risk symptomatic patients would prevent ICA in patients with a normal coronary CTA. In the setting of acute chest pain in the emergency department, patients can be rapidly and effectively triaged in addition to excluding extracardiac causes of chest pain. It is conceivable, however, that coronary CTA may result in an increase in the number of unnecessary ICA procedures and subsequent revascularizations. This was seen in a recent study in which more patients in the coronary CTA arm underwent ICA and subsequent revascularization than did those treated with the standard of care. 49 Although requiring further validation, the diagnosis of flow- limiting CAD by coronary CTA may identify patients who warrant intensified risk factor modification and goal-directed medical therapy. Additionally, individuals with flow-limiting CAD by coronary CTA will likely be referred for additional diagnostic testing, possibly ICA with revascularization, especially in the setting of left main coronary artery or multivessel disease.
Cost-effectiveness of cardiac CT in symptomatic individuals
There are limited data that suggest that coronary CTA appears to be a time- and cost-effective strategy in patients presenting with acute chest pain to the emergency room. Coronary CTA has been shown to significantly reduce the median diagnostic time in patients undergoing MDCT angiography (3.4 versus 15 hours) compared with patients treated with the standard of care. Reduced cost is primarily a result of reduced length of stay. 49 Although this study does not show cost-effectiveness, it suggests a potential cost-effective approach if applied across large numbers of patients presenting to emergency departments annually for acute chest pain.
In symptomatic persons with stable chest pain, CTA has been shown to be cost-effective in individuals with low-to-intermediate pretest likelihood of CAD (<50%) as compared with traditional diagnostic modalities, such as ICA, stress echocardiography, and exercise treadmill tests. In individuals with higher pretest likelihood, ICA was more cost-effective. 52
Contraindications and limitations of cardiac CT
Multiple contraindications to performing cardiac CT exist relating to patient safety and potential artifacts. Because of the need for iodinated contrast agents, cardiac CT should be avoided in individuals with intravenous contrast allergies and renal insufficiency. There is a small but non-negligible risk of contrast-induced nephropathy; however, it is associated with high in-hospital morbidity and mortality. 53 Radiation exposure has been linked to malignancy and birth defects. Consequently, women who are pregnant or breastfeeding should not undergo cardiac CT. With the widespread use of cardiac CT for the detection of subclinical coronary artery atherosclerosis, this has become an issue, especially in young women because of the risk of breast cancer. A recent study reported the estimated lifetime risk attributable to a single coronary CTA to be as high as 1 in 143 for a 20-year-old woman. 54 Additionally, obese patients require increased X-ray tube current output for adequate tissue penetration and spatial resolution and thus receive a higher radiation dose.
Factors that lead to artifact include arrhythmias (atrial fibrillation or flutter and premature ventricular or arterial contractions), heart rate >65 beats per minute that is refractory to beta-blockade, 55,56 metallic structures (vascular clips, bypass graft anastomosis markers, and metallic valves), dense calcium, coronary artery stents, body mass index (BMI) >40 kg/m 2 , and poor opacification.
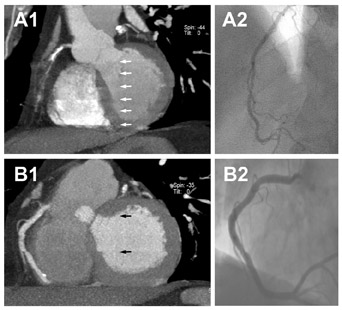
As a result of blooming artifacts (caused by partial-volume effect resulting in a brighter appearance adjacent to the calcium), calcium in the vessel wall obscures the lumen and reduces the ability to detect stenosis. Multiple studies have shown the deleterious effects of CAC on diagnostic accuracy as a result of increasing the percent of unevaluable segments, resulting in lower sensitivities and specificities. 57-59 Metal objects, such as vascular clips, are also susceptible to X-ray scatter, resulting in streak artifacts. Extreme obesity results in excessive radiation attenuation with subsequent reduction in signal-to-noise ratio. Examples of these artifacts are illustrated in Figure 5. Newer technology using DSCT has been shown to reduce the effect of calcification on image quality. 60
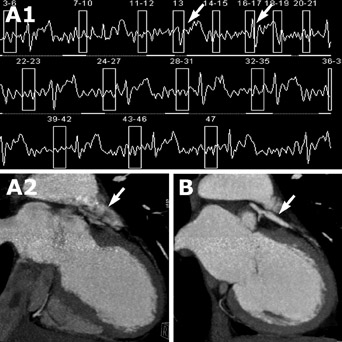
Cardiac motion artifacts are a major cause of image degradation. Heart rate irregularity results in slice misregistration. Similarly, poor gating can result in slice misregistration artifact. This artifact can be minimized through image reconstruction techniques. Figure 6 shows an example of a patient before and after correction for inappropriate gating. Typical reconstruction intervals are at 60% of diastole, although the optimal reconstruction interval providing the least amount of motion may vary by patient and vessel. An example of optimizing image quality by changing the reconstruction interval is illustrated in Figure 7. Initial feasibility studies using 256-slice CT have shown the ability to perform the entire study in 1 cardiac cycle without electrocardiographic gating, thus potentially eliminating artifacts from heart rate variability. 61 Fast heart rates cause image blurring (Figure 8). Beta-blockers are typically given to achieve an optimal heart rate <65 bpm. With improved technology, such as DSCT, higher heart rates may be acceptable, thereby eliminating the need for heart rate control. 60,62
In addition to potential artifacts, a significant limitation of this technology is that cardiac CT provides only the presence and extent of atherosclerosis but does not assess for myocardial ischemia. Nor at the present time does cardiac CT provide prognostic information regarding long-term cardiovascular morbidity and mortality. In contrast, stress testing (such as myocardial perfusion imaging) offers both evaluation for ischemic burden as well as the associated prognostic implications. Current efforts to use hybrid-imaging techniques, such as single-photon emission CT (SPECT)/CT and positron emission tomography (PET)/ CT are being developed and potentially could provide near-simultaneous anatomic and physiologic information. An initial feasibility study has shown improved diagnostic accuracy with hybrid SPECT/CT when compared with MDCT alone. 63
Professional society recommendations
The exact role of cardiac CT has not been fully elucidated, and the guidelines are evolving. A recent scientific statement published by the AHA suggests that there is conflicting evidence and diverging opinions about the usefulness of cardiac CT for the detection of coronary artery atherosclerosis. According to the AHA guidelines, CAC assessment is useful for the detection of subclinical CAD in intermediate-risk asymptomatic individuals. For symptomatic persons, coronary CTA is useful in those with low-to-intermediate pretest likelihood of CAD. 64 Additionally, several imaging societies have collaborated on the 2006 Appropriateness Criteria for Cardiac CT Imaging. 65 According to this consensus statement, the usefulness of CAC measurement is uncertain in asymptomatic individuals. Coronary CTA is considered to be appropriate for the evaluation of both stable angina and acute chest pain in individuals with intermediate pretest probability of CAD. 65 The usefulness of coronary CTA in patients following revascularization is uncertain in symptomatic individuals and is considered to be inappropriate in asymptomatic individuals.
Future directions
Although promising, cardiac CT still has limitations that prevent a broad clinical application in the detection of coronary artery atherosclerosis. In addition, it is a problem that no large trials have firmly established its clinical utility, cost-effectiveness, or the best way to integrate cardiac CT in the work-up of patients with suspected CAD. Multiple technologic advancements on the horizon (including DSCT, 256slice MDCT, and hybrid imaging with PET-CT or SPECT-CT) will offer the potential for reduced artifacts and for an overall improvement in diagnostic accuracy. On-going randomized trials are evaluating the potential applications of coronary CTA in the evaluation of acute chest pain. The future is bright for cardiac CT as a potential mainstay of noninvasive imaging of coronary arteries.
Acknowledgements
I would like to thank Drs. Pamela Woodard and Robert Gropler for their mentorship and Drs. Santosh Mathews, Suraj Kurup, Michael Barry, Brian Seeck, and Peter Rao for their constructive criticism of the manuscript.
Related Articles
Citation
Cardiac CT for coronary artery atherosclerosis detection: Potential applications in symptomatic and asymptomatic individuals. Appl Radiol.
December 17, 2007