Splenogonadal fusion
Images





Splenogonadal fusion. (The urologist felt there was no indication for surgical intervention at the time and decided to closely observe the patient as follow-up).
The differential diagnosis includes malignant testicular tumor, adenomatoid tumor, epididymitis, hemangioma and hematoma.
Findings
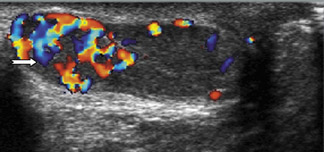
Testicular ultrasound revealed a solid, hypervascular mass in the left scrotum, which may either be intratesticular or paratesticular in nature.The possibility of splenogonadal fusion was entertained, based on the extremity anomalies and a 99mTc sulfur-colloid examination was suggested for further evaluation.
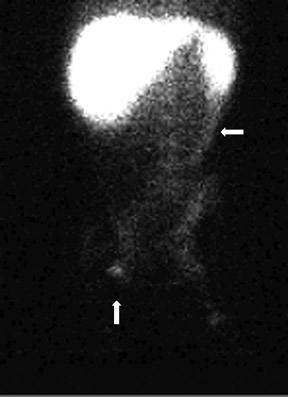
The99mTc sulfur colloid scan (Figure 3) demonstrated evidence of functional hyposplenia and focal activity in the left scrotum, suggesting ectopic reticulo-endothelial or possibly splenic tissue. A track of activity was also noted to extend from the spleen to the left scrotum.
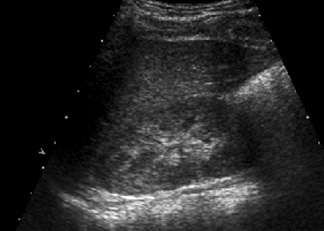
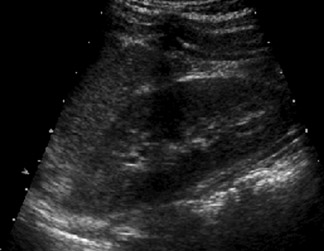
A renal ultrasound (Figure 4) that was performed a year earlier was within normal limits. Magnetic resonance imaging (MRI) of the spine was also performed, when the patient was 3 months old, and the spinal cord was not found to be tethered.
Discussion
Splenogonadal fusion is a rare congenital anomaly that affects both sexes, with a male-to-female ratio of 16:1. It was first described in 1889 and about 150 cases have been reported in the English literature.1 In males, the left testicle, or other derivatives of the mesonephros, connect to splenic tissues, usually an accessory spleen. In females, a similar fusion occurs between the left ovary and splenic tissue.
The condition is classified into two types: continuous (56%) and discontinuous (44%). In the continuous type, a strand of tissue directly connects the the spleen and gonad, whereas, there is no anatomic connection between the gonadal tissue and the spleen in the discontinuous type.2
The malformation in males manifests as a testicular mass, and the diagnosis is seldom made preoperatively. A definite diagnosis cannot be made solely on sonographic findings and the use of99mTc sulfur colloid scintigraphy to identify splenic tissue (either accessory or native) activity adds more information to the imaging diagnosis.3 Surgical exploration is however, required to exclude malignancy, since the accessory spleen that is attached to the testicle may be misinterpreted as a primary, malignant testicular tumor or an adenomatoid tumor.
Patients often exhibit congenital anomalies that include limb defects; reduction deformity of the arms and forearms; no digits or missing digits on the hands; reduction deformity of the legs; hind legs; no digits or missing digits on the feet; spinal dysraphism; congenital diaphragmatic hernia; lung hypoplasia or lung agenesis; thoracopagus; micrognathia; microgastria; craniostenostosis; anal atresia or anal stenosis;hypoplasia; and, polysplenia.
The discontinuous type usually is not associated with congenital defects.
CONCLUSION
Splenogonadal fusion is a rare congenital anomaly. The malformation in males manifests as a testicular mass, and surgical exploration is required to exclude malignancy. However, unnecessary orchiectomy can be avoided because splenic tissue can be dissected away from the tunica albuginea.
- Imperial SL, Sidhu JS. Nonseminomatous germ cell tumor arising in splenogonadal fusion. Arch Pathol Lab Med. 2002;126:1222-1225.
- Putschar WG, Manion WC. Splenicgonadal fusion. Am J Pathol. 1956;32:15-33.
- Guarin U, Dimitrieva Z, Ashley SJ. Splenogonadal fusion-a rare congenital anomaly demonstrated by 99Tc-sulfur colloid imaging: Case report. J Nucl Med. 1975;16:922-924.
Citation
. Splenogonadal fusion. Appl Radiol.
May 19, 2009