Radiological Case: Placental cyst
Images



CASE SUMMARY
A 28-year-old, gravida 2, para 1 woman presented in her second trimester for routine sonographic evaluation. Her obstetrical history was unremarkable. The routine blood tests were normal.
IMAGING FINDINGS
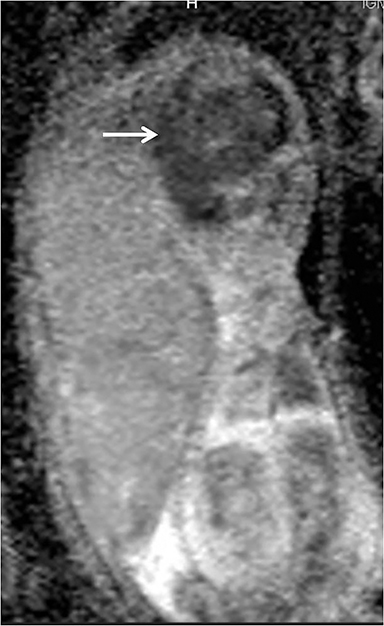
Sonography revealed a single fetus with normal growth parameters. However, there was placentomegaly with a thickness of 6.5cm and a large, thin-walled cyst on the placental fetal surface abutting the umbilical cord insertion. No solid component or blood flow was appreciable in the cyst. An MRI scan was performed after 2 days to evaluate the contents of the placental cyst; the images revealed fluid-fluid level suggestive of hemorrhage which was not seen in previous ultrasound imaging (Figure 1). The fetal head showed scalp edema and intracranial extra-axial hemorrhage (Figures 1 and 2) with diffusion restriction in fetal brain (Figures 3 and 4). Fluid-fluid level was also seen in the amniotic fluid (Figures 1 and 2). The patient aborted the dead fetus the following day. The amniotic fluid was blood stained. The placental cyst had ruptured and could not be delineated separately from partially necrosed placenta.
DIAGNOSIS
Placental cyst
DISCUSSION
The placenta may show various types of cystic structures, which can be broadly categorized into septal cysts, in which the cysts are located within placental tissue, and the more rarely encountered subchorionic, or true placental cysts, which are located under the fetal plate.1 These cysts are usually single but may be multiple. True placental cysts are rare with a prevalence of 2% to 7%.2 Their etiology is unknown, but they are more common in diabetes or in cases of maternofetal rhesus incompatibility. These cysts are usually asymptomatic, with the most common complication being intrauterine growth retardation. Their location near the cord site may lead to umbilical cord constriction and compromise of fetal blood flow. Rarely, these cysts may cause intrauterine fetal asphyxia and death.3
CONCLUSION
Placental cysts near the cord insertion site should be monitored sonographically and any feature suggestive of fetal hypoxia warrants timely intervention.
REFERENCES
- Raga F, Ballester MJ, Osborne NG, et al. Subchorionic placental cyst: A cause of fetal growth retardation-ultrasound and color-flow Doppler diagnosis and follow-up. J Natl Med Assoc.1996; 88:285-288.
- Elsayes KM, Trout AT, Friedkin AM, et al. Imaging of the placenta: A multimodality pictorial review. RadioGraphics. 2009; 29:1371–1391.
- Brown DL, DiSalvo DN, Frates MC, et al. Placental surface cysts detected on sonography histologic and clinical correlation. J Ultrasound Med. 2002;21:641–646.
Citation
Radiological Case: Placental cyst. Appl Radiol.
September 2, 2015