Radiological Case: Cystic lymphangioma
Images
CASE SUMMARY
A previously healthy 33-year-old female presented with a two-week history of right lower-quadrant pain.
IMAGING FINDINGS
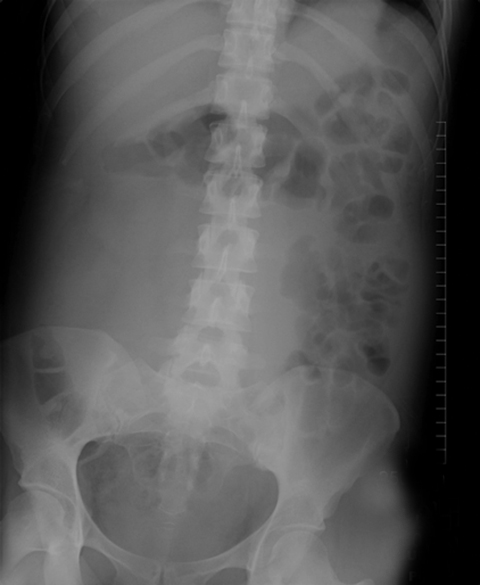
Abdominal radiograph (Figure 1) demonstrates increased soft-tissue density in the right abdomen with displacement of bowel gas,which is suspicious for an underlying mass.
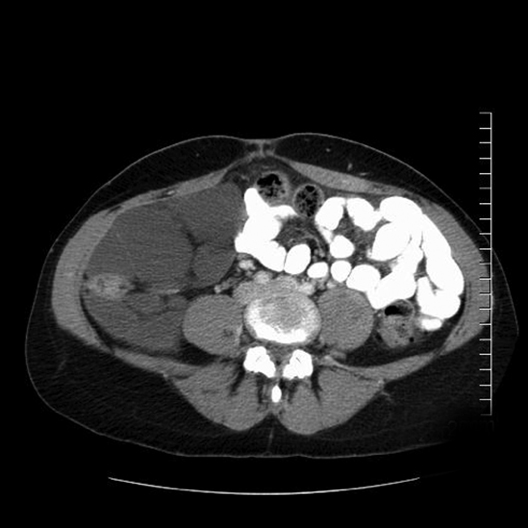
Contrast-enhanced computed tomography (CT) of the abdomen and pelvis (Figure 2) shows a multilocular fluid-density retroperitoneal mass that fills the right abdomen and encases the right colon. Thin septations are present. No nodules are seen.
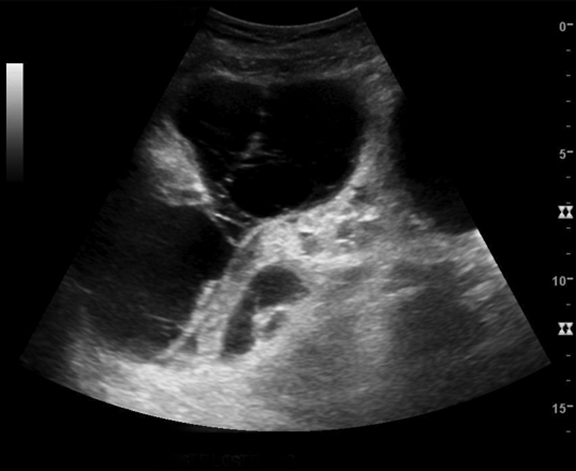
Ultrasound (Figure 3) confirms a multiseptated cystic mass in the right abdomen surrounding the right colon.
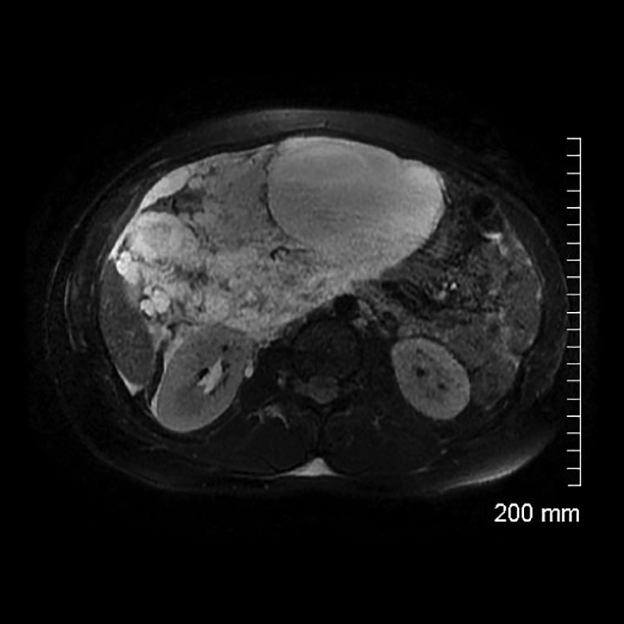
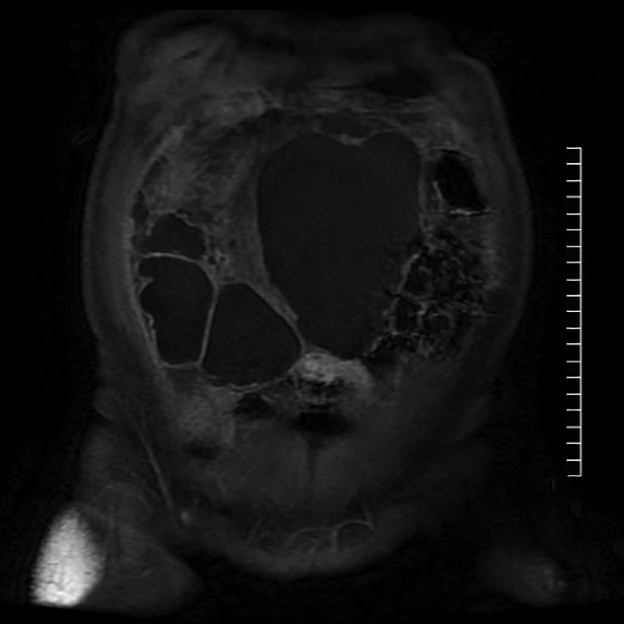
Magnetic resonance imaging (MRI) (Figures 4 and 5) performed 9 days after the CT demonstrates interval enlargement of the multiloculated fluid signal mass, which now crosses midline. The mass effect on the right ureter results in mild right hydronephrosis, new from the prior CT. Postcontrast images demonstrate enhancement of the thin septations without nodularity.
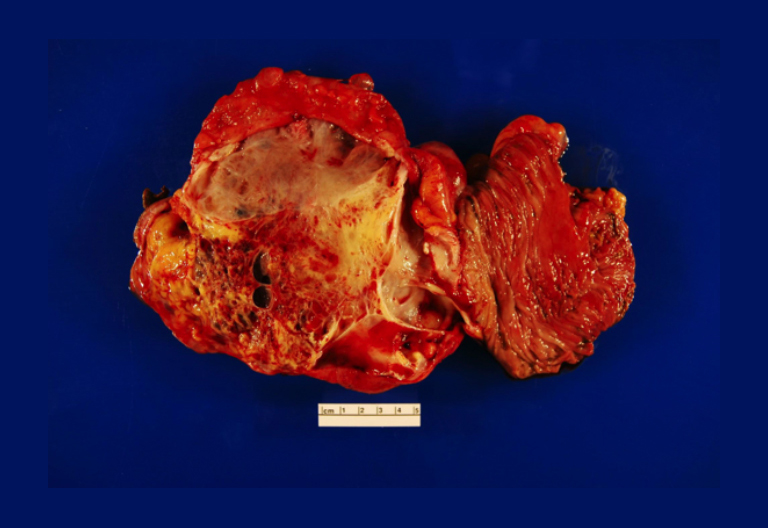
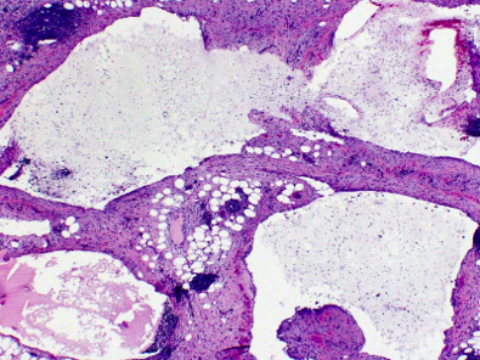
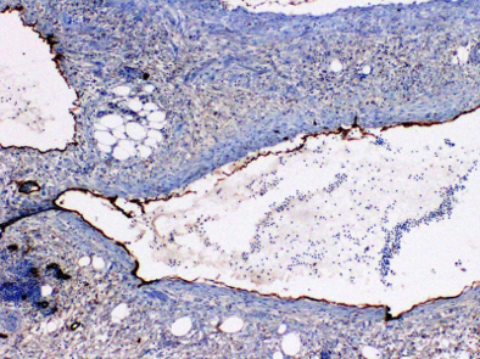
Gross specimen following surgical resection shows the multilocular cystic mass attached to the right colon (Figure 6). A microscopic evaluation demonstrates flattened epithelial cells lining the cysts (Figure 7). Abundant lymphocytes with lymphoid aggregates are presentin the cyst walls and septa. The cyst linings are positive for D2-40 by immunohistochemistry, indicating lymphatic endothelium (Figure 8).
DIAGNOSIS
Retroperitoneal cystic lymphangioma. The differential diagnosis based on imaging findings included cystic mesothelioma andvretroperitoneal cystadenoma.
DISCUSSION
Cystic lymphangiomas are rare congenital masses which are thought to be caused by failure of developing lymphatic tissue to establish a normal communication with the remainder of the lymphatic system. These abnormal lymphatic channels then dilate to form aunilocular or multilocular cystic mass.1 Of all cystic lymphangiomas, 95% occur in the neck and axillary region. Less common locations include the mesentery, retroperitoneum, abdominal viscera, lung, and mediastinum.2 When retroperitoneal, cystic lymphangiomas tend to cross into adjacent anatomic compartments.3
Retroperitoneal lymphangiomas occur in patients of all ages without sex predilection.1 Patients are commonly symptomatic and often present with abdominal distention, palpable mass, and/or pain.4 These clinical symptoms usually result from the compression of adjacent structures. Pain may also result from inflammation or hemorrhage into the mass.5 They are treated with surgical excision, though the insinuating nature of the lesion may make complete excision difficult in some cases.2 Resection of the adjacent bowel may be necessary.
Abdominal radiographs characteristically show displacement of bowel gas by a soft tissue mass.1 Cross-sectional imaging confirms the predominantly fluid nature of the mass, which is often multilocular. Sonography generally demonstrates multilocular cystic masses with thin internal septae. The cysts can be anechoic or contain echogenic debris.4 CT shows large, thin-walled, multiseptate cystic masses.3 Wall calcification can rarely be seen.1 On MRI, the signal pattern follows that of fluid (low T1, high T2). Contrast-enhanced studies may show enhancement of the cyst wall and septae.2
Following excision, gross specimens demonstrate thin-walled cystic masses that may contain chylous, serous, hemorrhagic,or mixed fluid.2 On microscopic examination, the cysts are lined with attenuated endothelial cells, similar to those of normal lymphatic tissue. The surrounding stroma is composed of collagen and fibrous tissue that contains scattered aggregates of lymphoid tissue.1
In the case presented, follow-up MRIs at 6 and 11 months following surgical resection showed no residual or recurrent mass.
CONCLUSION
Retroperitoneal cystic lymphangiomas are rare congenital masses that frequently are symptomatic secondary to mass effect on the gastrointestinal and genitourinary systems. Imaging demonstrates multilocular cystic masses with thin septations that frequently cross into adjacent compartments.
REFERENCES
- Davidson AJ, Hartman DS. Lymphangioma of the retroperitoneum: CT and sonographic characteristics. Radiology. 1990; 175:507-510.
- Levy AD, Cantisani V, Miettinen M. Abdominal lymphangiomas: Imaging features with pathologic correlation. AJR. 2004;182:1485-1491.
- Yang DM, Jung DH, Kim H, et al. Retroperitoneal cystic masses: CT, clinical, and pathologic findings and literature review. Radiographics. 2004;24:1353-1365.
- Ros PR, Olmsted WW, Moser RP, et al. Mesenteric and omental cysts: Histologic classification with imaging correlation. Radiology. 1987;164:327-332.
- Iyer R, Eftekhari F, Varma D, et al. Cystic retroperitoneal lymphangioma: CT, ultrasound and MR findings. Pediatr Radiol. 1993;23:305-306.
Citation
Radiological Case: Cystic lymphangioma . Appl Radiol.
June 5, 2014