Peripheral arteriovenous malformations: Classification and endovascular treatment
Images





In this review we cover the classification and endovascular management of arteriovenous malformations (AVMs). We begin by viewing AVMs in relation to the broader class of congenital vascular malformations and subsequently go into more depth on the clinical and pathologic characteristics that define AVMs. We then focus on the endovascular treatment options for peripheral AVMs and summarize the functional characteristics of the sclerosants and embolic agents available to clinicians today.
Vascular malformations and their classification
Arteriovenous malformations (AVMs) are abnormal shunts between arteries and veins that result from disturbances in angiogenesis. They are high-flow malformations that are radiographically characterized by a central nidus, a tangle of blood vessels where the abnormal arterial-venous communication exists without a normal intervening capillary bed. They can arise anywhere in the body and therefore have a wide range of presentations, from an asymptomatic birthmark to a life-threatening impingement on vital structures. Typically present at birth, they grow concomitantly with the patient and may be stimulated to grow further after periods of trauma, hormonal change, infection or spontaneous hemorrhage. Historically, surgical resection has been considered the treatment of choice. However, due to the significant morbidity and high rate of recurrence associated with surgical resection, endovascular therapy has emerged as a less invasive alternative with comparable efficacy.1
AVMs fall within the broader category of congenital vascular malformations (CVMs), which are any abnormal blood vessels arising from disturbed angiogenesis. CVMs can involve any portion of the vascular tree, including veins, arteries, capillaries, lymphatics or any combination thereof. Unlike vascular tumors, CVMs generally do not exhibit abnormalities in cellular proliferation.
Two main classification systems are used to describe CVMs: Mulliken and Hamburg. The Mulliken system divides CVMs into either high flow or low flow. This is a practical and useful classification since high flow lesions are treated with catheter-directed embolization and low flow lesions are treated with percutaneous sclerotherapy. The Hamburg system distinguishes vascular malformations based on their predominant histological components (lymphatic, arterial, venous, etc.). It divides each type into truncular, arising from the normal vascular tree, or extra-truncular, arising from outside the vascular tree. Truncular lesions arise from disturbances later in angiogenesis than extra-truncular and, in regard to treatment, tend to be higher flow than extra-truncular. In 2014, the International Society for the Study of Vascular Anomalies combined the Hamburg and Mulliken systems and also expanded on each of them (Table 1).2 CVMs are now separated into four categories based on clinical context and vessel involvement.
Clinical staging
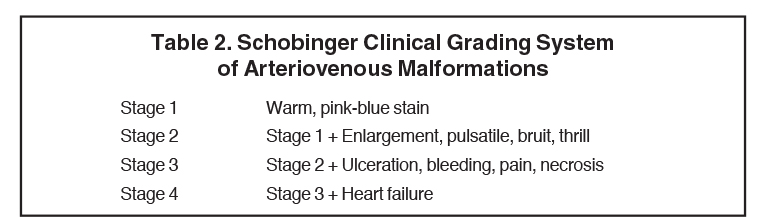
The Schobinger classification is a clinical assessment of vascular shunting that is predictive of treatment success (Table 2).3 This classification has four stages, with stage 1 lesions being asymptomatic and stage 4 representing high-output heart failure. Stages 2 and 3 are intermediate, with stage 3 lesions demonstrating ulceration, bleeding, pain, and necrosis. In general, Schobinger stage 3 lesions and above should receive treatment.4 Whether lower stage AVMs should be treated is still up for debate. One study found that almost all AVMs at Schobinger stage 1 eventually progressed, with nearly half becoming stage 3 and above. The authors, therefore, recommended early treatment regardless of stage.4
Imaging findings in AVMs
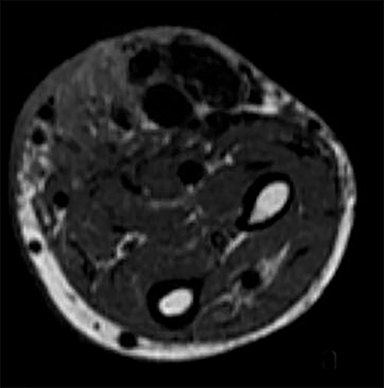
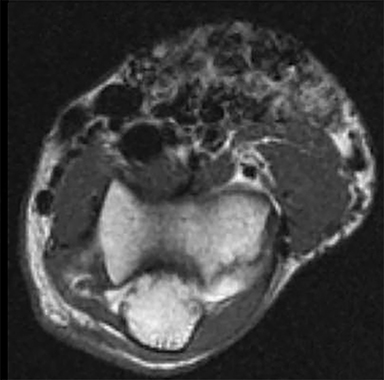
Initial imaging tests should include Doppler ultrasound and CT with contrast, or MRI. On Doppler, one may observe arterial waveforms and high flows in venous structures which are indicative of vascular shunting.5 MRI will often show a conglomerate of flow voids on T1- and T2-weighted images that may not respect soft tissue planes (Figure 1.6 Time-resolved MRA has emerged as a useful tool, not only to delineate nidal anatomy, but also to assess treatment efficacy through the measurement of venous filling times.7 CT angiography is an alternative to MRA that gives comparable images; however, the 3D reconstruction lacks temporal resolution.8 4D-CT angiography is an emerging technology that may be able to overcome this barrier and has shown to be useful for brain AVMs.9 In general, MRI and MRA are the preferred primary imaging modalities as they deliver both excellent anatomical resolution of the AVM and surrounding soft tissue, which are necessary for analyzing the extent of peripheral AVMs.
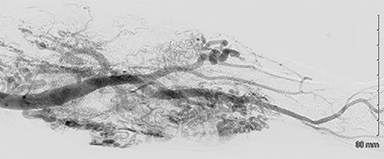
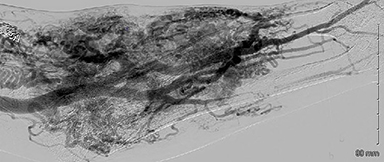
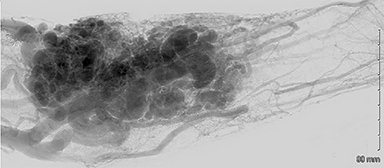
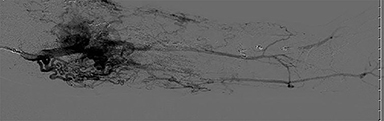
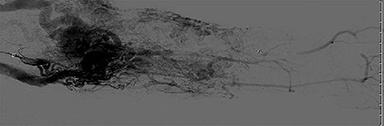
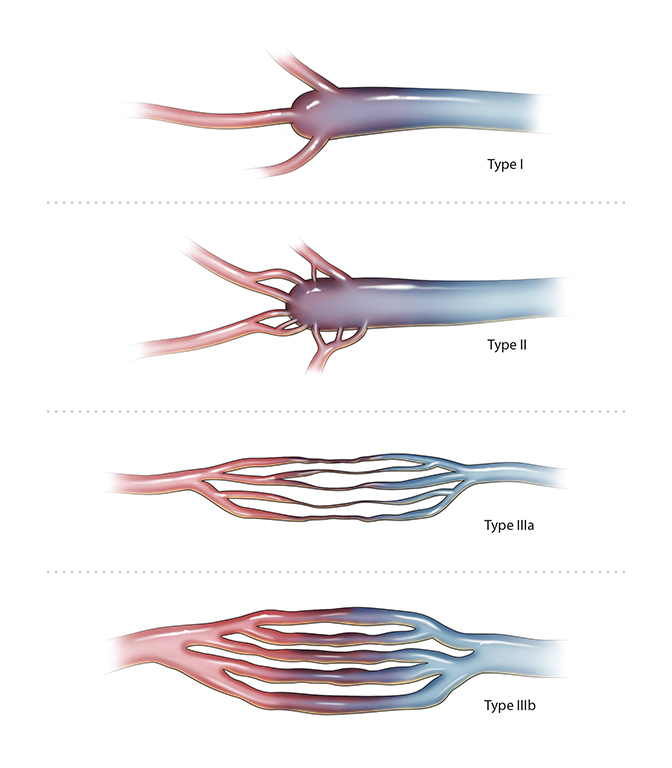
Diagnostic angiography should be performed on almost all AVMs and is absolutely required prior to treatment to assess flow rate, visualize anatomy of the nidus in greater detail than MRA and identify vessels required for distal circulation (Figure 2).10 AVMs can be identified as a tangled mass of blood vessels with early venous filling. If performed during embolization, accessory feeder vessels may begin to be visualized as primary feeder vessels are embolized.7 The architecture of the nidus on angiography has implications for treatment and outcomes. Cho described four distinct nidal architectures and found that AVMs consisting of multiple feeders emptying into a single vein, type 1 and 2, have the best response to treatment (Figure 3). AVMs with multiple inflows and outflows, types 3a and 3b, have the worst response.11
Endovascular treatment options
Embolic materials
Several embolic materials are available for endovascular treatment of peripheral AVMs. These embolic materials include: ethanol, N-butyl cyanoacrylate (NBCA), poly-vinyl-alcohol (PVA) particles, ethylene vinyl alcohol copolymer (Onyx), and endovascular coils and vascular plugs. Each one has specific handling criteria and learning curves. It is often the case that multiple different embolics are used to treat a single AVM. Detergents such as ethanoloamine oleate, polidocanol, and sotradecol have been reported, but are generally avoided because of increased recurrence risk.
Ethanol is widely regarded as the most effective liquid embolic. It directly damages the endothelium by acting as a protein denaturant, denuding the vessel to the internal elastic lamina. It is cost effective, but carries higher rates of complications such as significant edema, skin necrosis and nerve damage. Therefore, it should be diluted to 50% or not used at all in AVMs involving significant portions of skin.12,13 The most-feared complication from ethanol is the dose-dependent risk of pulmonary hypertension and cardiovascular collapse, which necessitates intraprocedural pulmonary arterial pressure (PAP) monitoring.14 PAP begins to increase with doses higher than 0.14mL/kg and the maximum recommended dose per treatment session is 0.5 – 1mL/kg administered in small 1 – 3cc aliquots; many administer less than 0.5mL/kg.15 PAP above 25mmHg systolic merit treatment with nitroglycerin infusion at 1mcg/kg/min.16 PAP is found to peak 10 to 15 minutes post-operatively; therefore patients must be monitored closely.17 Outflow occlusion reduces the increase of PAP and should be employed whenever possible. Finally, ethanol is very painful and general anesthesia is required. Ethanol can be mixed with iodized oil (Lipiodol) if visualization is desired.6
N-butyl cyanoacrylate is a liquid casting adhesive agent generally considered to be safer than ethanol. It may be preferred in AVMs with large, draining veins that would require great amounts of ethanol or Onyx, or in the pediatric population where ethanol dosing needs to be limited.18,19 It polymerizes quickly and irreversibly when exposed to anions and is effective in the setting of coagulopathy.20 To administer, ingredients are mixed in a glass vial and only polypropylene syringes and catheters (Tru-Fill recommends the Prowler, Prowler Select or Transit family of catheters) may be used. To minimize premature polymerization, NBCA should diluted with non-ionic solvent (Lipiodol) and the catheter flushed with 5% dextrose solution. The catheter used for angiography may also be used for embolization if perfectly flushed, but some opt to use a new catheter. The ratio of NBCA to Lipiodol is determined based on lesion flow dynamics, with more concentrated NBCA being used for higher flow lesions. In our experience, an NBCA-to-Lipiodol ratio of 1:3 is a good starting point with an expected polymerization time of 1-4 seconds. Exact casting time is difficult to predict and may lead to complications such as embolizing too proximal or having the catheter become glued into the vessel lumen.21 Operators should allow an adequate buffer zone so the catheter can be slowly withdrawn during administration. Adequate visualization is paramount as the operator must watch for any reflux of the embolic. Another method to prevent reflux is to “push” an aliquot of n-BCA out of the catheter with D5W allowing deeper penetration into the AVM and away from the catheter tip. If the catheter becomes adhered, a quick tug followed by prolonged traction often will remove it. However, if unsuccessful, an open removal may be necessary.
Ethylene vinyl alcohol copolymer (Onyx) is another liquid casting agent with an extensive track record for safety and efficacy in treatment of central nervous system AVMs. It has many of the same applications as nBCA and is gaining in popularity because it is easier to use.22, 23 Solubilized in DMSO, it polymerizes from outside in allowing further penetration into the nidus. It is injected slowly; the maximum injection rate is 0.1mL/min to avoid vasospasm caused by DMSO. Like NBCA, the viscosity and casting time can be changed by varying the concentration. 6-8% are the typical concentrations for adequate distal penetration from intra-arterial access. However in high flow fistulous malformations concentrations as high as 20% may be needed to achieve adequate casting time.22 Using a test injection of contrast to determine the amount of Onyx to use is inaccurate due to the differences in viscosity and changes in flow rate during injection of the embolic. If reflux is seen around the catheter, administration should be stopped for up to 2 minutes to allow the refluxed Onyx to solidify. Afterward administration can be resumed. In the event of reflux, the catheter may be dislodged by aspirating whilst applying constant, gentle traction. It may take several seconds to dislodge and the cast may stretch up to 3 cm during this period, but this is normal. The primary advantage of Onyx over NBCA is the slow flow and longer casting time, giving the operator greater control over administration. The downside is longer treatment times and greater expense. In superficial lesions, it may cause “tattooing” of the skin.
PVA particles may be used on rare occasions to de-vascularize a lesion either as a pre-surgical adjunct or in the management of an acutely bleeding AVM. However, this carries a high risk of complications related to non-target embolization due to selection of improper particle size. Authors have used particle sizes from 150 – 500 um.24,25 There are several reported cases of pulmonary embolism after PVA embolization.26,27 We do not recommend the use of PVA particles in the management of AVMs except for in the most experienced hands and only for the above mentioned indications.
Endovascular coils and vascular plugs have a limited role in the treatment of peripheral AVMs. Their major drawback is their size which may limit future vascular access if subsequent embolization is required. They have been used as stand-alone therapy exclusively in pulmonary and renal AVMs where the large diameter and simple architecture are amenable to such treatment.21 As an adjunct, coils and vascular plugs are useful agents for outflow occlusion, especially in nidi with a dominant outflow vein.19,28 Especially in very high flow AVMs, coils may sometimes may be displaced and migrate, posing a potential embolic risk; however, this is not commonly reported.29
Treatment techniques
The goal of AVM embolization is to obliterate the nidus while simultaneously minimizing non-target embolization. This can be best achieved by slowing the flow to improve operator control and intra or juxtanidal positioning of the catheter (Figure 4). The techniques to achieve these goals depend on AVM nidal architecture as well as anatomic location. We will organize treatment approaches based on the angiographic classification developed by Cho (Figure 3).30
In AVMs with a dominant outflow vein, types one and two, retrograde or direct puncture have become the preferred methods of access. Flow is first reduced either via manual occlusion of the draining vein or blood pressure cuff. For lesions not amenable to the above methods, such as those in the trunk, balloon occlusion of the inflow or outflow may be useful. In large aneurysmal draining veins, coils and glues have been successfully used to occlude the outflow.28, 31 In small AVMs of this type NBCA alone has been shown to be potentially curative.32 In most cases though, after the outflow is occluded, retrograde filling of the nidus can be achieved either with ethanol or Onyx.19,28,33,34 Operators are cautioned when using high amount of outflow occlusion as sclerosant can reflux into the arterial system if injected too quickly.
For AVMs with multiple feeders and outflows, types 3a and 3b, a trans-arterial or direct puncture approach is recommended.30 Direct puncture may be necessary in situations where the tortuosity of the arterial feeder precludes juxtanidal positioning or when the operator is unable to assess proper positioning of the catheter in very complex AVMs.12 This may be difficult and time-consuming for small vessels and runs the risk of sclerosant.35,36 Flow occlusion continues to be paramount to ensure adequate contact time with the nidus. Manual compression of the draining vein or a blood pressure cuff should be employed when possible. A combination approach has been described using a trans-arterial NBCA injection to slow flow followed by direct puncture of sclerosant into nidal vessels.35
At our institution, we first perform catheter-based diagnostic angiography with selective and super-selective catheter positioning using compression adjuncts when appropriate. For all but the most simple AVMs, we then bring the patient back for staged treatment. In the interim, the patient’s history, physical exam findings and MRI and angiographic images are reviewed by a team that includes interventional radiology, diagnostic radiology, plastic surgery and vascular surgery.
Postoperative pain and swelling should be expected and can sometimes be significant. The use of perioperative corticosteroids to control postoperative swelling is not well studied, but is recommended by those with considerable experience treating these lesions.37 Patients are typically seen in clinic once a month after treatment begins, sooner if indicated, until the primary endpoint of symptomatic relief is reached or further endovascular treatment is precluded due to anatomical or clinical considerations.
Outcomes
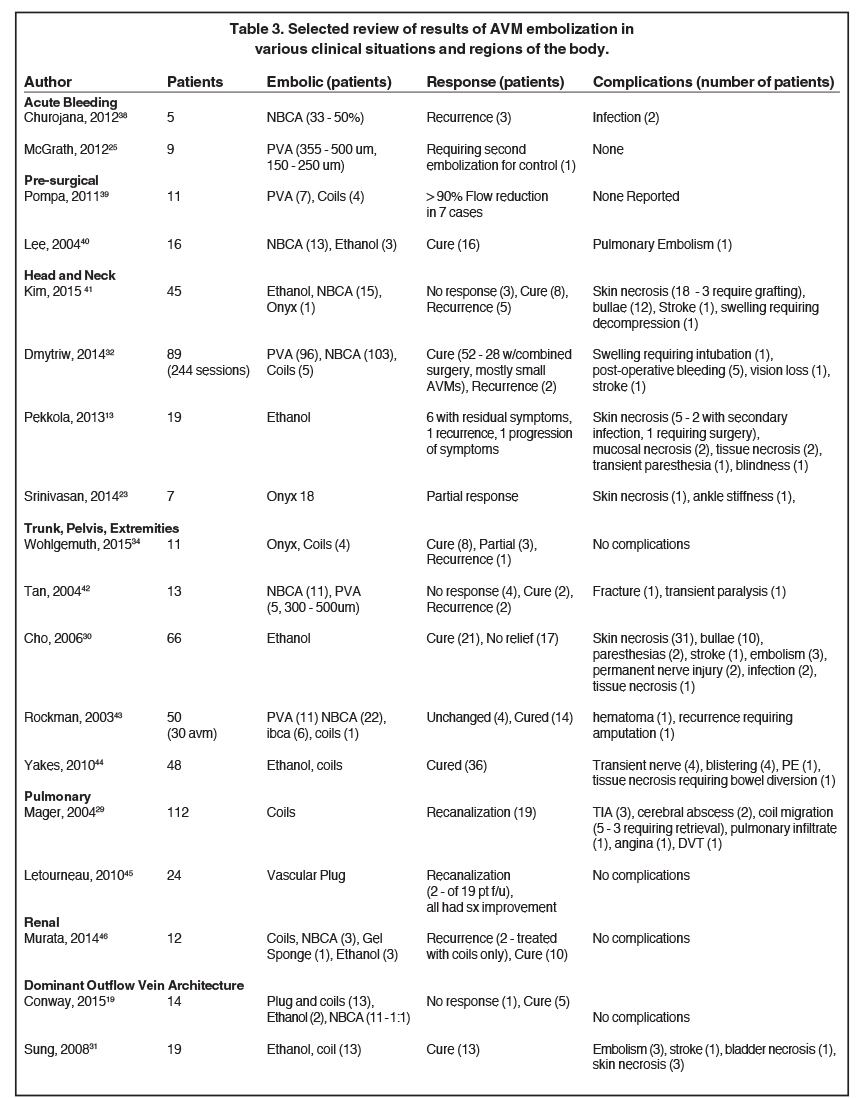
There is limited data on the treatment of peripheral AVMs with most reports being small case series. Outcomes vary considerably mostly due to the heterogeneous nature of AVMs. Large, diffuse AVMs are often not curable and embolotherapy is merely palliative.11 Small AVMs, especially those with a single outflow vein, have a high chance of cure with embolotherapy alone.32 However, if treated correctly, most patients will experience at least symptomatic improvement after endovascular therapy. Recurrence is a common problem, especially if prior treatment resulted in loss of preferred methods of access. Table 3 provides a selected review of the literature on various AVMs.
Conclusion
Peripheral AVMs have myriad manifestations, and treatment depends on the acuity of the situation, nidal architecture and anatomic location. Treatment is often a long process requiring multiple rounds of embolization and lifelong follow up. We emphasize the use of a multidisciplinary team and to personalize treatment to the patient’s wishes, as currently there is no cure. We have provided a description of treatment techniques, complications and outcomes associated with various sclerosants. We also describe our institutional techniques and literature based techniques for treating these lesions. Larger, controlled studies are needed to provide more robust data on the safety, efficacy, treatment techniques, and periprocedural management of these patients.
References
- 1. Hyodoh H, Hori M, Akiba H, et al. Peripheral vascular malformations: Imaging, treatment approaches, and therapeutic issues. Radiographics. 2005;25 Suppl 1:S159-171.
- ISSVA Classification of Vascular Anomalies ©2014 International Society for the Study of Vascular Anomalies. https://s3.amazonaws.com/ClubExpressClubFiles/298433/documents/issva_classification_2014_final_trial.pdf?AWSAccessKeyId=AKIAIB6I23VLJX7E4J7Q&Expires=1436810557&response-content-disposition=inline%3B%20filename%3Dissva_classification_2014_final_trial.pdf&Signature=k0PV0BKQ7%2FGhsys8%2Flz1kRqsV0I%3D. Accessed May 1, 2017.
- Kohout MP, Hansen M, Pribaz JJ, et al. Arteriovenous malformations of the head and neck: Natural history and management. Plast Reconstr Surg. 1998;102(3):643-654.
- Liu AS, Mulliken JB, Zurakowski D, et al. Extracranial arteriovenous malformations: Natural progression and recurrence after treatment. Plast Reconstr Surg. 2010;125(4):1185-1194.
- Dubois J, Garel L. Imaging and therapeutic approach of hemangiomas and vascular malformations in the pediatric age group. Pediatr Radiol. 1999;29(12):879-893.
- Legiehn GM, Heran MK. Classification, diagnosis, and interventional radiologic management of vascular malformations. Orthop Clin North Am. 2006;37(3):435-474, vii-viii.
- Mulligan PR, Prajapati HJS, Martin LG, et al. Vascular anomalies: classification, imaging characteristics and implications for interventional radiology treatment approaches. Br J Radiol. 2014;87(1035):20130392.
- Bittles MA, Sidhu MK, Sze RW, et al. Multidetector CT angiography of pediatric vascular malformations and hemangiomas: utility of 3-D reformatting in differential diagnosis. Pediatr Radiol. 2005;35(11):1100-1106.
- Willems PW, Taeshineetanakul P, Schenk B, et al. The use of 4D-CTA in the diagnostic work-up of brain arteriovenous malformations. Neuroradiology. 2012;54(2):123-131.
- Herborn CU, Goyen M, Lauenstein TC, et al. Comprehensive time-resolved MRI of peripheral vascular malformations. AJR Am J Roentgenol. 2003;181(3):729-735.
- Park KB, Do YS, Kim DI, et al. Predictive factors for response of peripheral arteriovenous malformations to embolization therapy: Analysis of clinical data and imaging findings. J Vasc Interv Radiol. 2012;23(11):1478-1486.
- Vogelzang RL, Atassi R, Vouche M, et al. Ethanol embolotherapy of vascular malformations: clinical outcomes at a single center. J Vasc Interv Radiol. 2014;25(2):206-213; quiz 214.
- Pekkola J, Lappalainen K, Vuola P,et al. Head and neck arteriovenous malformations: Results of ethanol sclerotherapy. AJNR Am J Neuroradiol. 2013;34(1):198-204.
- Ko JS, Kim JA, Do YS, et al. Prediction of the effect of injected ethanol on pulmonary arterial pressure during sclerotherapy of arteriovenous malformations: Relationship with dose of ethanol. J Vasc Interv Radiol. 2009;20(1):39-45.
- Shin BS, Do YS, Cho HS, et al. Effects of repeat bolus ethanol injections on cardiopulmonary hemodynamic changes during embolotherapy of arteriovenous malformations of the extremities. J Vasc Interv Radiol. 2010;21(1):81-89.
- Lee BB, Do YS, Byun HS, et al. Advanced management of venous malformation with ethanol sclerotherapy: Mid-term results. J Vasc Surg. 2003;37(3):533-538.
- Ko JS, Kim CS, Shin BS, et al. Changes in pulmonary artery pressures during ethanol sclerotherapy for arteriovenous malformations: identifying the most vulnerable period. Clin Radiol. 2011;66(7):639-644.
- Lungren MP, Patel MN. Endovascular management of head and neck vascular malformations. Curr Otorhinolaryngol Rep. 2014;2(4):273-284.
- Conway AM, Qato K, Drury J. Embolization techniques for high-flow arteriovenous malformations with a dominant outflow vein. J Vasc Surg. 2015.
- Morishita H, Yamagami T, Matsumoto T, et al. Transcatheter arterial embolization with N-butyl cyanoacrylate for acute life-threatening gastroduodenal bleeding uncontrolled by endoscopic hemostasis. J Vasc Interv Radiol. 2013;24(3):432-438.
- Rosen RJ, Nassiri N, Drury JE. Interventional management of high-flow vascular malformations. Tech Vasc Interv Radiol. 2013;16(1):22-38.
- Numan F, Omeroglu A, Kara B, et al. Embolization of peripheral vascular malformations with ethylene vinyl alcohol copolymer (Onyx). J Vasc Interv Radiol. 2004;15(9):939-946.
- Srinivasan KG, Vidyadharan R, Patel N, et al. Embolisation of high flow extracranial/peripheral arteriovenous malformations (AVMs) with ethylene vinyl alcohol copolymer (ONYX®) in children - Birmingham Children’s Hospital experience. Eur J Plast Surg. 2014;37(3):129-134.
- Chen WL, Ye JT, Xu LF, et al. A multidisciplinary approach to treating maxillofacial arteriovenous malformations in children. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(1):41-47.
- McGrath S, Harding V, Lim AK, et al. Embolization of uterine arteriovenous malformations in patients with gestational trophoblastic tumors: A review of patients at Charing Cross Hospital, 2000-2009. J Reprod Med. 2012;57(7-8):319-324.
- Kjellin I, Boechat M, Vinuela F, et al. Pulmonary emboli following therapeutic embolization of cerebral arteriovenous malformations in children. Pediatr Radiol. 2000;30(4):279-283.
- Kline JN, Ryals TJ, Galvin JR, et al. Pulmonary embolization and infarction: An iatrogenic complication of transcatheter embolization of a cerebral arteriovenous malformation with polyvinyl alcohol sponge. Chest. 1993;103(4):1293-1295.
- Wang D, Su L, Han Y, et al. Ethanol embolotherapy of high-flow auricular arteriovenous malformations with electrolytically detachable coil-assisted dominant outflow vein occlusion. Eur J Vasc Endovasc Surg. 2014;48(5):576-584.
- Mager JJ, Overtoom TT, Blauw H, et al. Embolotherapy of pulmonary arteriovenous malformations: Long-term results in 112 patients. J Vasc Interv Radiol. 2004;15(5):451-456.
- Cho SK, Do YS, Shin SW, et al. Arteriovenous malformations of the body and extremities: Analysis of therapeutic outcomes and approaches according to a modified angiographic classification. J Endovasc Ther. 2006;13(4):527-538.
- Sung KC, Young SD, Dong IK, et al. Peripheral arteriovenous malformations with a dominant outflow vein: Results of ethanol embolization. Korean Radiol. 2008;9(3):258-267.
- Dmytriw AA, Ter Brugge KG, Krings T, et al. Endovascular treatment of head and neck arteriovenous malformations. Neuroradiology. 2014;56(3):227-236.
- Hernandez D. Transvenous embolization of arteriovenous malformation. 2012 http://www.nursinglibrary.org/vhl/handle/10755/243371?mode=full. Accessed May 1, 2017.
- Wohlgemuth WA, Müller-Wille R, Teusch VI, et al. The retrograde transvenous push-through method: A novel treatment of peripheral arteriovenous malformations with dominant venous outflow. Cardiovasc Intervent Radiol. 2015; 38(3); 623-631.
- Kitagawa A, Izumi Y, Hagihara M, et al. Ethanolamine oleate sclerotherapy combined with transarterial embolization using n-butyl cyanoacrylate for extracranial arteriovenous malformations. Cardiovasc Intervent Radiol. 2014;37(2):371-380.
- van der Linden E, van Baalen JM, Pattynama PM. Retrograde transvenous ethanol embolization of high-flow peripheral arteriovenous malformations. Cardiovasc Intervent Radiol. 2012;35(4):820-825.
- Lee BB, Baumgartner I, Berlien HP, et al. Consensus document of the International Union of Angiology (IUA)-2013 current concepts on the management of arterio-venous malformations. Int Angiol. 2013;32(1):9-36.
- Churojana A, Khumtong R, Songsaeng D, Chongkolwatana C, Suthipongchai S. Life-threatening arteriovenous malformation of the maxillomandibular region and treatment outcomes. Interventional neuroradiology: Journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2012;18(1): 49-59.
- Pompa V, Valentini V, Pompa G, Di Carlo S, Bresadola L. Treatment of high-flow arteriovenous malformations (AVMs) of the head and neck with embolization and surgical resection. Annali italiani di chirurgia. 2011;82(4):253-259.
- Lee BB, Do YS, Yakes W, Kim DI, Mattassi R, Hyon WS. Management of arteriovenous malformations: a multidisciplinary approach. Journal of vascular surgery. 2004;39(3):590-600.
- Kim B, Kim K, Jeon P, Kim S, Kim H, Byun JH, Kim D, Kim Y. Long-term results of ethanol sclerotherapy with or without adjunctive surgery for head and neck arteriovenous malformations. Neuroradiology.2015 Apr;57(4):377-86. doi: 10.1007/s00234-1483. Epub 2015 Jan 7.
- Tan KT, Simons ME, Rajan DK, Terbrugge K. Peripheral high-flow arteriovenous vascular malformations: a single-center experience. Journal of vascular and interventional radiology:JVIR. 2004;15(10):1071-1080.
- Rockman CB, Rosen RJ, Jacobowitz GR, Weiswasser J, Hofstee DJ, Fioole B, Lamparello PJ, Adelman MA, Gagne PJ, Riles TS. Transcatheter embolizationof extremity vascular malformations: The long-term success of multiple interventions. Ann Vasc Surg. 2003 Jul;17(4):417-23
- Yakes W. Abstract No. 200: Ethanol embolotherapy management of pelvic arteriovenous malformations. Journal of vascular and interventional radiology: JVIR. 2010;21(2):S77.
- Letourneau-Guillon L, Faughnan ME, Soulez G, et al. Embolization of pulmonary arteriovenous malformations with amplatzer vascular plugs: safety and midterm effectiveness. Journal of vascular and interventional radiology: JVIR. 2010;21(5):649-656.
- Murata S, Onozawa S, Nakazawa K, et al. Endovascular embolization strategy for renal arteriovenous malformations. Acta Radiol. 2014;55(1):71-77.
Citation
K L, A P, M R.Peripheral arteriovenous malformations: Classification and endovascular treatment. Appl Radiol. 2017; (5):15-21.
May 10, 2017