Part I: MR of the female pelvis
Images






Dr. Agrawal is a Nuclear Medicine Fellow, Division of Nuclear Medicine, Mallinckrodt Institute of Radiology, St. Louis, MO; Dr. Sethi is a Research Associate, Department of Radiology, and Dr. Oto is a Professor, Department of Radiology, Biological Sciences Division, University of Chicago, Chicago, IL.
The multiplanar capabilities and excellent soft-tissue contrast on magnetic resonance imaging (MRI) of the pelvis provide superb depiction of the female pelvic anatomy and often lead to specific diagnosis without ionizing radiation. MRI is often used as a problem-solving tool in patients where ultrasound is inconclusive or suboptimal. It is a modality of choice particularly for preoperative characterization and staging of endometrial and cervical cancer and, hence, it plays an important role in stratifying patients into appropriate treatment options. MR imaging is uniquely well suited to the evaluation of gynecologic conditions that occur during pregnancy and in the postpartum period. The development of new, faster imaging sequences with parallel imaging has enabled acquisition of images of a moving fetus and dynamic evaluation of the entire female pelvic floor.
The goal of this article is to familiarize the reader with techniques and applications of MR imaging in the female pelvis, including recent advances, and discuss imaging features of various abnormal conditions affecting the female pelvis.
MRI technique
Patient preparation
The patient should fast for at least 4 hours and empty the bladder and bowel just before examination to reduce blurring from motion artifacts and ghosting due to bowel peristalsis and bladder motion. Other measures may include antispasmodics, such as glucagon (0.5-1.0 mgIV/IM) or hyoscine butylbromide 20-40 mg IM/IV. Intravenous administration of these antiperistaltic agents has been shown to improve image quality and lesion visualization in oncological pelvic MRI and is recommended for routine use.1
MRI imaging protocol
A phase-array surface coil is used to increase signal-to-noise ratio (SNR). A basic imaging protocol must include a high-resolution, free-breathing T2W sequences in the axial, oblique sagittal, and coronal planes and an axial T1-weighted imaging (T1WI) sequence with and without fat suppression. Recently developed high-resolution 3-dimensional, T2-weighted images appear promising and may decrease total scan time. For benign disease, fast breath-hold sequences are often enough despite slightly decreased resolution. However, evaluating pelvic malignancies requires long duration, high-resolution, T2-weighted FSE sequences. Optional sequences include contrast-enhanced fat suppressed, T1WI. This can be obtained in dynamic fashion using 3-dimensional GRE-T1WI sequences. The fat-saturated T1WI sequence is specifically necessary to characterize fat or hemorrhage within the adnexa when there is a clinical suspicion of dermoid or endometriosis.Other optional sequences depending on indication include diffusion imaging, dynamic contrast-enhanced MRI,2 and peristalsis and pelvic-floor imaging.
Diffusion-weighted imaging improves not only the detection and potentially the characterization of small uterine tumors and complex ovarian cancer, but also the visualization of small implants of peritoneal carcinomatosis, which could significantly impact patient management. ADC measurement may be useful for monitoring the therapeutic outcome after uterine arterial embolization (UAE), chemotherapy and/or radiation therapy.3-8
DCE-MRI has the potential to improve tumor detection and local staging, and can also provide quantitative information about tumor perfusion, which may be useful for both monitoring therapeutic effects and predicting therapeutic outcome.9
Protocols should be optimized and tailored to address a specific indication for pelvic imaging. Optimal protocol for a specific condition will be discussed further in the text when each condition is addressed in detail.
Normal uterine anatomy on MRI imaging
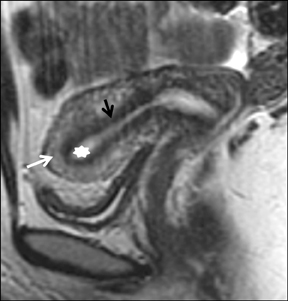
The uterus can be divided into the uterine corpus and cervix. On T1WI the entire uterus is isointense to muscle and different anatomic zones cannot be identified. The premenopausal uterine corpus on T2-weighted images (T2WI) show 3 distinct zones (Figure 1):
- The central high-signal intensity endometrium and secretions measure 3 to 6 mm in the proliferative phase and 5 to 13 mm in the secretory phase.
- The middle low-signal intensity junctional zone measures 2 to 8 mm and is the innermost layer of myometrium (less water, more smooth muscle and greater percentage of nuclear area). The appearance of the junctional zone changes with sustained myometrial contractions or uterine peristalsis are important to distinguish from leiomyomas or adenomyosis.
- The outer intermediate-signal intensity of the myometrium.
The postmenopausal uterus has an indistinct zonal anatomy, and the junctional zone is not consistently visualized. It should be kept in mind that Tamoxifen intake may induce endometrial hyperplasia, polyps, and carcinomas.
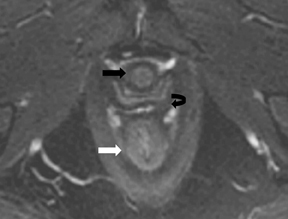
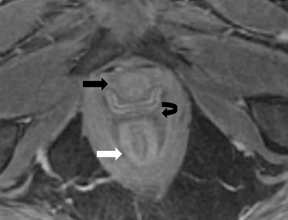
Cervix on T2WI shows the following distinct zones (Figure 1):
- Central hyperintense mucous
- High-signal intensity endocervical mucosa and glands (contains numerous folds and clefts as the plicae palmate). Combined thickness of zones 1 and 2 is 2 to 3 mm
- Hypointense fibrous stroma is 3 to 8-mm thick
- Outer intermediate signal intensity loose stroma
Congenital uterine anomalies
These occur in almost 1% of women within the reproductive age group. Although hysterosalpingography and ultrasound may suggest aMüllerian duct anomaly, further evaluation with MRI is often required, especially for complex cases. MRI is the best imaging method available because of its superior ability to reliably visualize and characterize complex uterovaginal anatomy. For evaluation of uterine anomalies, coronal oblique fast spin echo T2-weighted images parallel to the long axis of the uterine corpus are very useful.10-11
Uterine agenesis or hypoplasia may or may not be a small uterine remnant without identifiable zonal anatomy.
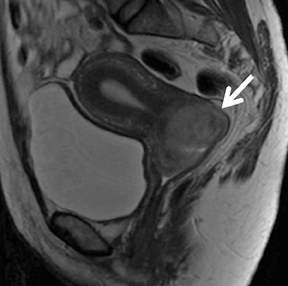
Unicornuate uterus has a reduced uterine volume, but normal endometrial—myometrial width ratio with a banana-shaped configuration of uterus (Figure 2). A rudimentary horn with or without endometrium may be present and may or may not show communication with the uterine cavity. Urologic anomalies like ipsilateral renal agenesis and ipsilateral pelvic kidney are often associated with unicornuate uterus.
Bicornuate uterus results from incomplete fusion of the uterine horns. On MR imaging, a fundal indentation deeper than 1 cm and a muscular and fibrous septum separating the divergent uterine horns greatly favors a bicornuate over septate uterus. When the septum extends all the way down to the cervix, causing its duplication, it is called bicollis, while it is a unicollis when septum does not reach the external os.
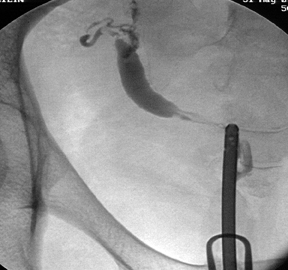
Uterus didelphys results from the arrest of midline fusion of Mullerian ducts and is characterized by complete/partial duplication of the uterus, cervix, and vagina. Patients are usually asymptomatic until menarche, unless obstruction is present. This may lead to hematocolpos, hematometra, and hematosalpinx. MR imaging demonstrates 2 widely separated horns and 2 cervices. The zonal anatomy is preserved in each hemiuterus (Figure 3).
Septate uterus results from the failure of resorption of the fibrous septum between the Mullerian ducts. MRI shows a fibrous septum, arising in the midline fundus, and variable in length. It is considered complete when it extends to the external cervical os. In approximately 25%of cases, the septum can extend to the upper vagina. The external uterine contour may be convex, flat, or mildly (<1.0 cm) concave and the indentation of the myometrium or septum into the endometrial canal is more than 1 cm.
Arcuate uterus is often considered a normal variant and not a congenital uterine anomaly. On MRI, the normal external uterine contour is maintained. There is smooth, broad and minimal indentation of myometrium or fibrous component into the endometrial canal (<1 cm).12, 13
Benign uterine conditions
Endometrial hyperplasia usually occurs in perimenopausal women, women taking estrogen without progesterone, women takingTamoxifen for breast cancer, or those with estrogen secreting tumors like granulosa cell tumors. Endometrial biopsy is diagnostic and is needed to exclude malignant transformation, which can be seen in 1% to 22% cases.14 MR imaging is helpful when transvaginal sonography is indeterminate and biopsy is limited by difficult anatomy or cervical stenosis. T2-weighted images demonstrate diffuse thickening of endometrial stripe, which appears iso- to slightly hypointense, compared with normal endometrium.
Endometrial polyps are typically seen in postmenopausal women. These may be asymptomatic or associated with irregular/persistent bleeding. On T2-weighted images, they can be readily distinguished from submucosal leiomyomas by their appearance. They are isointense or slightly hypointense to normal endometrium. The presence of a stalk or cystic area favors polyp over carcinoma or hyperplasia. Polyps show pronounced early enhancement that persist on delayed imaging compared to carcinoma, which shows only mild enhancement.
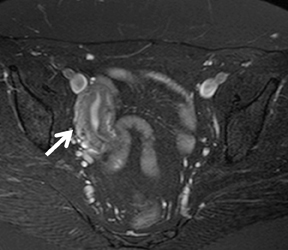
Leiomyomas are the most common benign uterine tumors and are usually asymptomatic, but symptoms may range from abnormal bleeding to mass effect, infertility, second trimester abortions, torsion, infection, acute degeneration, or sarcomatous degeneration. They can be classified by their location into submucosal, intramural, subserosal, or cervical. Ultrasound is often used for the diagnosis. MR imaging provides amore accurate determination of location, number, size, and degree of degeneration (Figure 4). These features are important for selecting patients before minimally-invasive treatments. MR imaging also evaluates arterial supply before UAE to assess for parasitized ovarian arteries that may lead to a poor response. MRI can also be helpful in identification of fibroids with a stalk, malignancy, and adenomyosis. On MRI, leiomyomastypically are well circumscribed, isointense to muscle on T1-weighted images, and homogeneously hypointense on T2-weighted images. A thin hyperintense rim of dilated lymphatic clefts, dilated veins, and edema may be seen on T2-weighted images and helps differentiate leiomyomas from focal adenomyosis. This rim may enhance with gadolinium administration.
Leiomyomas with degeneration may show heterogeneous high-signal intensity on T2-weighted images with lack of contrast-enhancement. Hemorrhagic (red) degeneration of pregnancy or after uterine artery embolization demonstrates high-signal areas on T1-weighted images. MR imaging is also very accurate in differentiating a subserosal leiomyoma from an ovarian tumor. A mass that is homogenously low-signal intensity on T2 is likely to be a leiomyoma and the only ovarian tumors that could mimic this appearance are ovarian fibroma and Brenner’s tumor; also benign lesions.15 The dynamic-contrast MR enhancement rate is higher for uterine leiomyomas than for ovarian fibromas in terms of both maximal enhancement (P < 0.001) and enhancement rate at 30 (P = 0.009), 60 (P = 0.007), and 90 seconds (P =0.0009).16
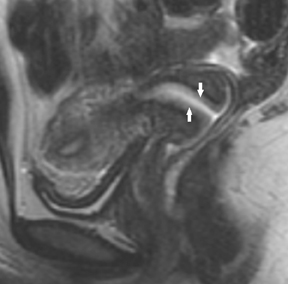
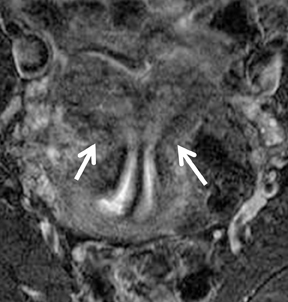
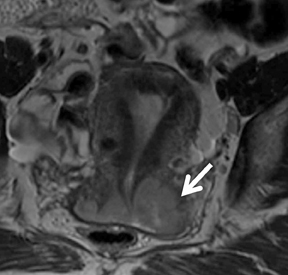
Adenomyosis constitutes endometrial stroma and glands within the myometrium in women of reproductive age and may be microscopic, focal (adenomyoma), or diffuse. Adenomyosis is usually asymptomatic, but may cause pain and dysfunctional uterine bleeding. MR imaging is a highly accurate noninvasive technique for the diagnosis with a high sensitivity (78% to 88%) and specificity (67% to 93%).17,18 On T2-weighted images, there is a thickening of the junctional zone to 12 mm or more. There may be either diffuse or focal thickening of the junctional zone forming an ill-defined area of low-signal intensity, occasionally with embedded bright foci on T2-weighted images (Figure 5). The presence of tiny hyperintense foci representing small deposits of ectopic endometrium, cystically dilated endometrial glands, or hemorrhagic fluid on T2-weighted images is pathognomonic of adenomyosis. If extensive hemorrhage is present, the imaging reveals larger, well-circumscribed, myometrial cysts containing blood products of different ages. Contrast-enhanced sequences may show uniform enhancement or a speckled appearance, with numerous nonenhancing foci corresponding to the punctate hyperintensities seen on T2-weighted images.
Differentiating both of these conditions is important, as it changes the treatment. Focal adenomyoma has characteristic features including a poorly defined border, minimal mass effect on the endometrium compared to a leiomyoma of same size, an elliptical rather than round configuration, may display linear striations radiating out from endometrium, and shows no dilated vessels at the margin of the lesion.19
Benign disease of the cervix
Nabothian cysts are the most common benign cervical lesions and are usually asymptomatic despite growth as large as 4 cm. These are caused by distension of endocervical glands or cleft with mucus. MR imaging demonstrate well defined margins and very high signal intensity lesions on T2-weighted images. Solid components within the cyst should raise suspicion for malignancy.
Cervical leiomyomas are easily distinguished by their well-defined margin and low signal intensity on T2-weighted images.
Endocervical polyps appear on MRI as a cystic or solid polypoidal mass within the lumen that protrudes into the endometrial cavity.
Malignant uterine disease
Endometrial carcinoma is the most common malignancy of the female genital tract that primarily occurs in postmenopausal women (sarcomas account for 2% to 5% of uterine malignancy). Ninety percent are adenocarcinoma; others types include adenocarcinoma with squamous differentiation, clear cell or papillary serous carcinoma. It is primarily staged surgically. MR imaging may greatly optimize the surgical procedure and therapeutic strategy. The role of MRI in endometrial cancer includes the evaluation of depth of myometrial invasion,cervical invasion, and nodal metastasis.
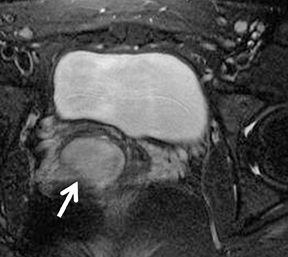
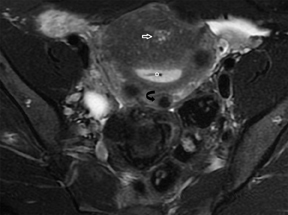
The spectrum of MRI findings include thickening of endometrium, foci of either low or high-signal intensity on T2-weighted images with less enhancement than the surrounding myometrium (Figure 6). Myometrial invasion is assessed based on thickness of the remaining myometrium (Table 1). Caution should be paid in the presence of adenomyosis, which can lead to diagnostic confusion.
Malignant disease of cervix
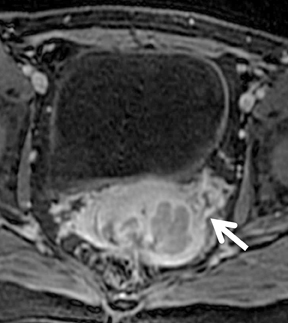
Cervical cancer is the second most common gynecological malignancy worldwide. The International Federation of Obstetrics and Gynecology (FIGO) (Table 2) recommends clinical staging based on physical exam, lesion biopsy, chest radiography, cystoscopy, and sonography if indicated. This approach has inherent inaccuracies (34%-39% discrepancy between clinical and surgical staging) in advanced stage disease and does not address nodal involvement. MR imaging has proven to be an excellent modality to evaluate tumor size, extent, and nodal involvement(Figure 7).21
The real strength of MR imaging for cervical carcinoma is the high negative predictive value of 95% for parametrial invasion.23 A study has documented 100% negative predictive value of MR imaging for bladder or rectal invasion, suggesting that MR imaging can obviate invasive procedures, such as cystoscopy, proctoscopy, and sigmoidoscopy, and thus can reduce staging costs and morbidity.24 For the detection of advanced stage disease, sensitivities for MR imaging (53%) and CT (42%) are much higher than FIGO clinical staging (29%).25 With a criterion of a minimal axial diameter of more than 1 cm, improved accuracy of 93.0% with a sensitivity of 62.2% and specificity of 97.9%has been reported.26
Conclusion
Thorough knowledge of the spectrum of MR imaging features of various physiologic variations and pathologic conditions that affect the female pelvis is essential for establishing an accurate diagnosis and guiding further management. MR is a reliable staging method for preoperative assessment of endometrial and cervical carcinoma.
Part 2 of this article is available in the May 2012 issue on the Applied Radiology website: www.appliedradiology.com.
References
- Johnson W, Taylor MB, Carrington BM, et al. The value of hyoscine butylbromide in pelvic MRI. Clin Radiol. 2007;62:1087-1093.
- Punwani S. Contrast enhanced MR imaging of female pelvic cancers: Established methods and emerging applications. Eur J Radiol. 2011;78:2-11.
- Namimoto T, Awai K, Nakaura T, et al. Role of diffusion-weighted imaging in the diagnosis of gynecological diseases. Eur Radiol. 2009;19:745-760.
- Thomassin-Naggara I, Fournier LS, Roussel A, et al. [Diffusion-weighted MR imaging of the female pelvis]. J Radiol. 2010;91:431-438;quiz 439-440.
- Harry VN, Semple SI, Gilbert FJ, Parkin DE. Diffusion-weighted magnetic resonance imaging in the early detection of response to chemoradiation in cervical cancer. Gynecol Oncol. 2008;111:213-220.
- Takeuchi M, Matsuzaki K, Nishitani H. Diffusion-weighted magnetic resonance imaging of endometrial cancer: Differentiation from benign endometrial lesions and preoperative assessment of myometrial invasion. Acta Radiol. 2009;50:947-953.
- Inada Y, Matsuki M, Nakai G, et al. Body diffusion-weighted MR imaging of uterine endometrial cancer: Is it helpful in the detection of cancer in nonenhanced MR imaging? Eur J Radiol. 2009;70:122-127.
- Tamai K, Koyama T, Saga T, et al. The utility of diffusion-weighted MR imaging for differentiating uterine sarcomas from benign leiomyomas. Eur Radiol. 2008;18:723-730.
- Koyama T, Togashi K. Functional MR imaging of the female pelvis. J Magn Reson Imaging. 2007;25:1101-1112.
- Chandler TM, Machan LS, Cooperberg PL, et al. Mullerian duct anomalies: From diagnosis to intervention. Br J Radiol. 2009;82:1034-1042.
- Olpin JD, Heilbrun M. Imaging of Müllerian duct anomalies. Clin Obstet Gynecol. 2009;52:40-56.
- Troiano RN, McCarthy SM. Mullerian duct anomalies: imaging and clinical issues. Radiology. 2004;233:19-34.
- Agrawal G, Riherd JM, Busse RF, et al. Evaluation of uterine anomalies: 3D FRFSE cube versus standard 2D FRFSE. AJR Am J Roentgenol. 2009;193:W558-562.
- Kurman RJ, Kaminski PF, Norris HJ. The behavior of endometrial hyperplasia. A long-term study of “untreated” hyperplasia in 170 patients. Cancer. 1985;56:403–412.
- Murase E, Siegelman ES, Outwater EK, et al. Uterine leiomyomas: Histopathologic features, MR imaging findings, differential diagnosis, and treatment. Radiographics. 1999;19:1179-1197.
- Thomassin-Naggara I, Daraï E, Nassar-Slaba J, et al. Value of dynamic enhanced magnetic resonance imaging for distinguishing between ovarian fibroma and subserous uterine leiomyoma. J Comput Assist Tomogr. 2007;31:236-242.
- Bazot M, Cortez A, Darai E, et al. Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: Correlation with histopathology. Hum Reprod. 2001;16:2427-2433.
- Ascher SM, Arnold LL, Patt RH, et al. Adenomyosis: Prospective comparison of MR imaging and transvaginal sonography. Radiology. 1994;190:803-806.
- Tamai K, Togashi K, Ito T, Morisawa N, et al. MR imaging findings of adenomyosis: Correlation with histopathologic features and diagnostic pitfalls. Radiographics. 2005;25:21-40.
- Koyama T, Tamai K, Togashi K. Staging of carcinoma of the uterine cervix and endometrium. Eur Radiol. 2007;17:2009–2019.
- Van Nagell JR Jr, Roddick JW Jr, Lowin DM. The staging of cervical cancer: Inevitable discrepancies between clinical staging and pathologic findings. Am J Obstet Gynecol. 1971;110:973-978.
- Togashi K, Nishimura K, Sagoh T, et al. Carcinoma of the cervix: Staging with MR imaging. Radiology. 1989;171:245-251.
- Kaji Y, Sugimura K, Kitao M, Ishida T. Histopathology of uterine cervical carcinoma: Diagnostic comparison of endorectal surface coil and standard body coil MRI. J Comput Assist Tomogr. 1994;18:785-792.
- Rockall AG, Ghosh S, Alexander-Sefre F, et al. Can MRI rule out bladder and rectal invasion in cervical cancer to help select patients for limited EUA? Gynecol Oncol. 2006;101:244-249.
- Hricak H, Gatsonis C, Chi DS, et al. Role of imaging in pretreatment evaluation of early invasive cervical cancer: Results of the intergroup study American College of Radiology Imaging Network 6651-Gynecologic Oncology Group 183. J Clin Oncol. 2005;23:9329-9337.
- Kim SH, Kim SC, Choi BI, Han MC. Uterine cervical carcinoma: Evaluation of pelvic lymph node metastasis with MR imaging. Radiology. 1994;190:807-811.