Invasive Pulmonary Aspergillosis
Images

CASE SUMMARY
A 15-year-old with a history of renal transplant treated with immunosuppressive drugs presented with low-grade fever, malaise, and cough.
IMAGE FINDINGS
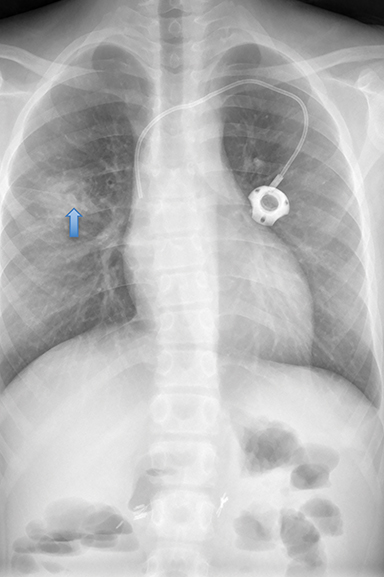
Initial chest radiograph demonstrated a right upper-lobe consolidation with a crescent shaped area of lucency (Figure 1). The air-crescent sign or Monad sign, is defined as a crescent-shaped gas collection that surrounds an intracavitary mass. The air-crescent sign in angioinvasive aspergillosis is a good prognostic indicator showing separation of the infarcted core from the granulation tissue. This differs from an aspergilloma, a fungus ball that forms in immune competent patients within a pre-existing lung cavity.1
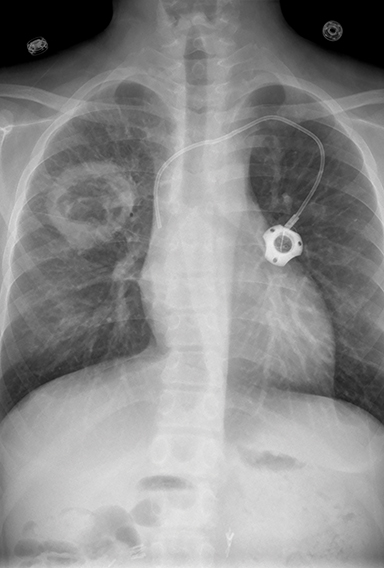
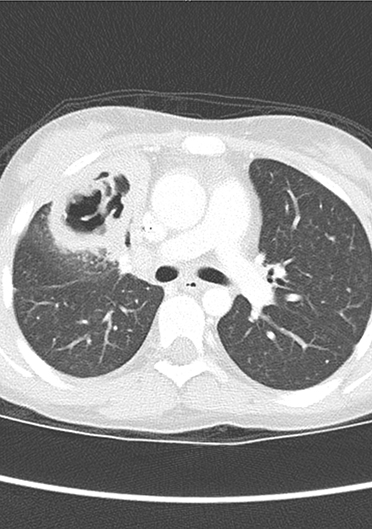
A follow-up chest radiograph 5 months later demonstrated evolution into a large, thick-walled cavity that had increased in size (Figure1). Chest CT at that time showed an irregular, thick-walled collection with a large, gas-filled cavity (Figure 2).
DIAGNOSIS
Invasive pulmonary aspergillosis (IPA).
The differential diagnosis of a child with a cystic or cavitary lung lesion is long and includes congenital and acquired lungs abnormalities. 1 Congenital cystic lesions include lobar emphysema, cystic adenomatoid malformations, pleuropulmonary blastoma, bronchogenic cyst, and pulmonary sequestration. Acquired lung lesions are classified as infectious, neoplastic, or of miscellaneous causes.
Among the most common infectious causes are bacterial and fungal infections, while parasitic infestations such as paragonimiasis and hydatidosis are rare outside of endemic areas. The more common organisms causing pulmonary cysts or pneumatoceles are Staphylococcus, Pseudomonas, Klebsiella, and anaerobes. Gram-negative bacteria, anaerobes, and occasionally Staphylococcus may cause lung abscesses.2
The more common chronic infections include tuberculosis, histoplasmosis, and coccidioidomycosis. These organisms are regionally prevalent and generally found in endemic regions or in travelers from these geographic locations. Neoplastic conditions that may have cystic lung disease as a feature are rare but include Langerhans cell histiocytosis and pleuropulmonary blastoma most commonly.2 Of the miscellaneous causes of pediatric cystic lung lesions, septic embolic, lung trauma/laceration, and hydrocarbon ingestion should be considered in the appropriate clinical setting.2
DISCUSSION
Aspergillus species are ubiquitous and normally found in the soil, where they play a role in carbon and nitrogen recycling. They form hardy spores that disperse into the air, causing a wide range of illnesses, depending on the immune status of the host. The most common human pathogens are A. flavus, A. terreus, and A. niger. Generally, people with competent immune systems do not develop clinical illness; however, individuals with immune deficiencies are most likely to develop pulmonary infections. Clinical manifestations of Aspergillus infection can be variable with increasing severity such as an aspergilloma, allergic bronchopulmonary aspergillosis, chronic necrotizing aspergillosis and invasive aspergillosis. The latter two presentations are typically seen in immunosuppressed individuals.
Children with long-standing asthma, and occasionally cystic fibrosis, may develop allergic bronchopulmonary aspergillosis (ABPA), a hypersensitivity reaction to fungal antigens. ABPA is a mild form of pulmonary aspergillosis representing an eosinophilic lung disease. ABPA is the result of hypersensitivity that develops from Aspergillus growing in the lumen of airways without invasion of the walls. Aspergillomas may form after multiple exposures to Aspergillus spores in an immune-competent host with a pre-existing cavitary lung lesion.
Invasive aspergillosis is the most severe form of the disease and is life threatening. The populations most at risk are those with immune suppression, such as children with congenital immunodeficiences and patients with acquired immune suppression secondary to chemotherapy for malignancies, transplants, or high-dose steroid therapy therapy.3-6 Signs and symptoms of infection include fever and chills, shortness of breath, bloody cough, chest or joint pain, and headaches.4 Infection may become disseminated as a result of hematogenous spread from the lungs to the brain, heart, kidneys, and skin.
In 2000, Wattier and Ramirz-Avila reported an incidence of invasive aspergillosis (IA) of about 0.4% of hospitalized immunosuppressed children.7 The groups at greatest risk were children undergoing hematopoietic stem cell transplants (4.5%), children treated for malignancies, especially acute myelogenous leukemia (4.0%), those with primary immunodeficiencies (6.5%), and children undergoing solid organ transplants (0.3%).8 In the pediatric population, pulmonary cavitary disease can result from acute or chronic infection, chronic disease, or malignancy. The clinical history and laboratory tests are helpful in refining the differential diagnosis.
The radiographic findings of IPA are variable. Initially, chest radiographs are often nondiagnostic or resemble the findings of asthma. Later, bronchiectasis may develop. In some cases, mucous plugs develop within the abnormal bronchi and appear as a sausage-shaped, “finger in a glove”. Chest CT is the most sensitive diagnostic modality for evaluating patients with IPA. Greater than 90% of patients have macronodules (>1 cm) and over 60% have a halo sign on CT. 9 The halo sign, a macronodule >1 cm surrounded by a perimeter of ground-glass opacity, is thought to be an early indicator of IPA. Other notable findings include wedge-shaped, pleural-based infarcts,10 pulmonary consolidations, cavities, and an air-crescent sign. Treatment may be initiated when a halo sign and/or macronodule are noted.
Strategies for preventing infection, as well as early diagnosis and therapy, are important for minimizing lung injury and preventing seeding of other organs. When IA is suspected, percutaneous biopsy/sampling of the walls of the cavity or fungus ball can confirm the diagnosis. Inserting a catheter into the cavity to directly infuse antifungal medications can also be useful. Surgical lobectomy may be considered in medically refractory cases.
For all types of Aspergillus, a lack of immune response is a critical issue and may be fatal. Complications affecting morbidity and mortality include airway blockage, respiratory failure, renal damage, and pulmonary hemorrhage. Invasive aspergillosis has a 30–90% mortality rate in immunocompromised patients.8,9
CONCLUSION
In an immunosuppressed patient, the presence of a pulmonary cavitary lesion should raise the concern for IPA.
REFERENCES
- Gaillard F. Air Crescent Sign (Apergilloma). Gaillard F. Radiopaedia. Accessed October 8.2020. https://radiopaedia.org/articles/air-crescent-sign-lung?lang=us,
- Odev K, Guler I, Altinok T, Pekcan S, Batur A, Ozbiner J. Cystic and Cavitary Lesions in Children: Radiologic Findings with Pathologic Correlation. J Clin Imaging Sci. 2013, 3:60; doi:10.4103/2156-7514.124087
- Nin, CS de Souza, VV Alves, GR et al. (2016). Solitary lung cavities: CT findings in malignant and non-malignant disease Clin Radiol, 71; 1132-1136 DOI: https://doi.org/10.1016/j.crad.2016.04.009 (epub ahead of print).
- Parkar AP, Kandiah P. Differential Diagnosis of Cavitary Lung Lesions. J Belg Soc Radiol. 2016;100(1):100. DOI: http://doi.org/10.5334/jbr-btr.1202
- Dagenais TRT, Keller NP. Pathogenesis of Aspergillus fumigatus in Invasive Aspergillosis. Clin Microbiol Rev. 2009;22;447-465. doi: 10.1128/CMR.00055-08
- Greene RE, Oestmann JW, Stark P, Durand C, Lortholary O, et al. Imaging Findings in Acute Invasive Pulmonary Aspergillosis: Clinical Significance of the Halo Sign. Clin Infect Dis.2007;44(3):373–379, https://doi.org/10.1086/509917.
- Wattier RL, Ramirez-Avilla L. Pediatric Invasive Aspergillosis. J Fungi. (Basel). 2016 Jun; 2(2): 19. doi: 10.3390/jof2020019
- Lin, SSchranz J, and Teutsch SM. Aspergillosis case-fatality rate: systematic review of the literature. Clin. Infect. Dis. 2001; 32:358-366.
- Franquet T, Müller NL, Giménez A, et al. Spectrum of Pulmonary Aspergillosis: Histologic, Clinical, and Radiologic Findings. RadioGraphics. 2001; 21:825–837.
Citation
J R, RB T, CM S, DJ A, AJ T.Invasive Pulmonary Aspergillosis. Appl Radiol. 2020; (6):46-48.
November 5, 2020