Hunter syndrome
Images

Hunter syndrome
Findings
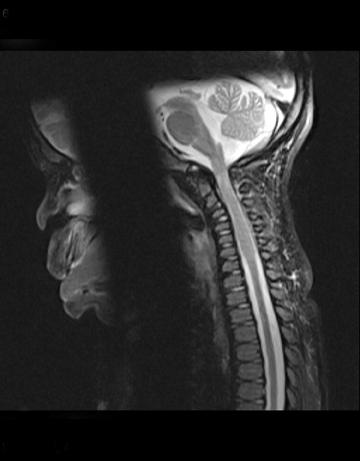
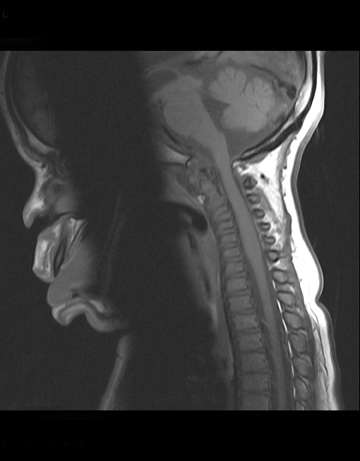
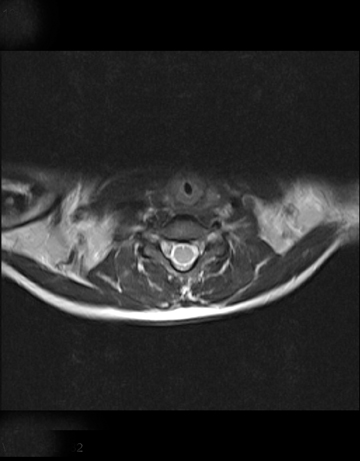
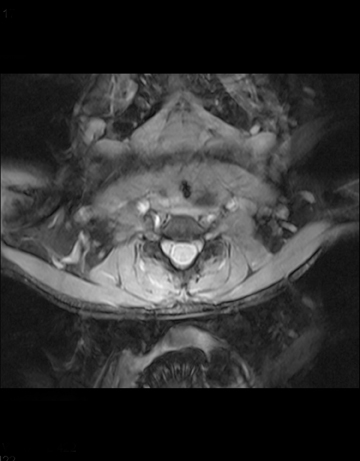
MRI of the cervical spine without contrast was available for review. The cervical spinal cord demonstrated moderate enlargement from the foramen magnum to C7, with a maximum caliber of 9 mm. Minimal diffuse T2 prolongation (Figure 1) was seen in the enlarged region without evidence of a focal mass or syrinx. The T1 signal (Figure 2) was normal. There was no evidence of an intradural, extramedullary lesion, or meningeal thickening. The thoracic cord was normal in caliber and signal, measuring 5 mm. The cervical spine (Figure 3) was normally aligned, and the dens was hypoplastic. Soft tissues posterior to the dens were prominent (Figure 4), measuring 3 mm in thickness and causing mild-to-moderate narrowing of the foramen magnum. Visualization of the brain (Figure 5) was limited to the inferior portions of the temporal and occipital lobes, but ventriculomegaly was noted, as was diffuse T2 prolongation throughout the visualized portions of white matter.
Discussion
Hunter syndrome is a genetic disorder classified as one of the lysosomal storage diseases, specifically mucopolysaccharidosis II. The buildup of glycosaminoglycans in the cells leads to symptoms early in life, generally in the first few years. The clinical features include macrocrania, distinct facial features, and usually developmental delay owing to the CNS involvement. Hepatosplenomegaly, joint problems, and airway compromise are also seen.1 Although typical clinical features are seen in the first few years of life, the diagnosis is made biochemically or with genetic testing.
The neuroradiologic findings are not specific, and they are commonly quite similar among the mucopolysaccharidoses. Although not necessarily useful diagnostically, imaging is suggestive, and may be used (as in this case) to evaluate a patient with changing neurologic symptoms.
Findings include macrocrania, dilated perivascular spaces, cystic spaces in the white matter, communicating hydrocephalus, and delayed myelination. Areas of T2 prolongation are therefore seen in the white matter.1 Thickening of the dura is noted as the cause of cervical spondylopathy in several cases in the literature.2-5 A search of Medline from 1966 to the present with the search words Hunter, mucopolysaccharidosis, thickening, cervical, and/or cord did not yield reports of cervical cord thickening in patients with Hurler syndrome.
Given that all cells have lysosomes, and that white matter involvement in the brain has been widely reported, it seems at least plausible that the cervical cord thickening seen in this patient is secondary to deposition of the mucopolysaccharide. Other diagnostic possibilities include astrocytoma, although this or other neoplastic processes would not likely have such a homogeneous appearance. In any case, biopsy of the cord was not performed.
In cases of cervical stenosis secondary to dural thickening, the treatment may include laminectomy and occipital craniotomy.2
Conclusion
In summary, Hunter syndrome is an uncommon mucopolysaccharidosis that frequently presents in early childhood with multisystem involvement. Typically, the cervical myelopathy has been attributed to extrinsic compression of the cord by thickened meninges. In the patient in question, dural thickening is not noted, but the presence of cervical cord thickening and T2 hyperintensity lead us to speculate that in this case the myelopathy is at least in part secondary to infiltration with mucopolysaccharides.
- Grossman, Robert I, Yoursem, David M. In: Neuroradiology: The Requisites. 2003. Philadelphia, PA, Elsevier.
- Kaendler S, Bockenheimer S, Grafin Vitzthum, H. Galow, W. Cervical myelopathy in mucopolysaccharidosis type II (Hunter’s Syndrome). Neuroradiologic, clinical and histopathologic findings (translated). Deutsche Medizinische Wohenschrift. 115:1348-1352.
- Ballenger, C E. Swift, T R. Leshner, R T. et al. Myelopathy in mucopolysaccharidosis type II (Hunter’s Syndrome). Annals of Neurology. 1980:7:382-385.
- Vinchon, M. Cotton, A. Clarisse, J. et al. Cervical myelopathy secondary to Hunter syndrome in an adult. AJNR Am J Neuroradiol. 1995;16:1402-1403.
- Koyama, K. Moda, Y. Sone, A. et al. Neurogenic bladder in Hunter’s syndrome. J Med Genetics. 1994; 31:257-258.