First Branchial Cleft Sinus
Images

CASE SUMMARY
An adult presented with swelling in the right periauricular region and recurrent episodes of suppuration previously treated with incision and drainage. They reported a single episode of purulent discharge from the right external auditory canal (EAC). Physical examination showed a painful and hard cervical mass at the inferior pole of the right parotid region, posterior to the angle of mandible. Otoscopy was bilaterally normal.
IMAGING FINDINGS
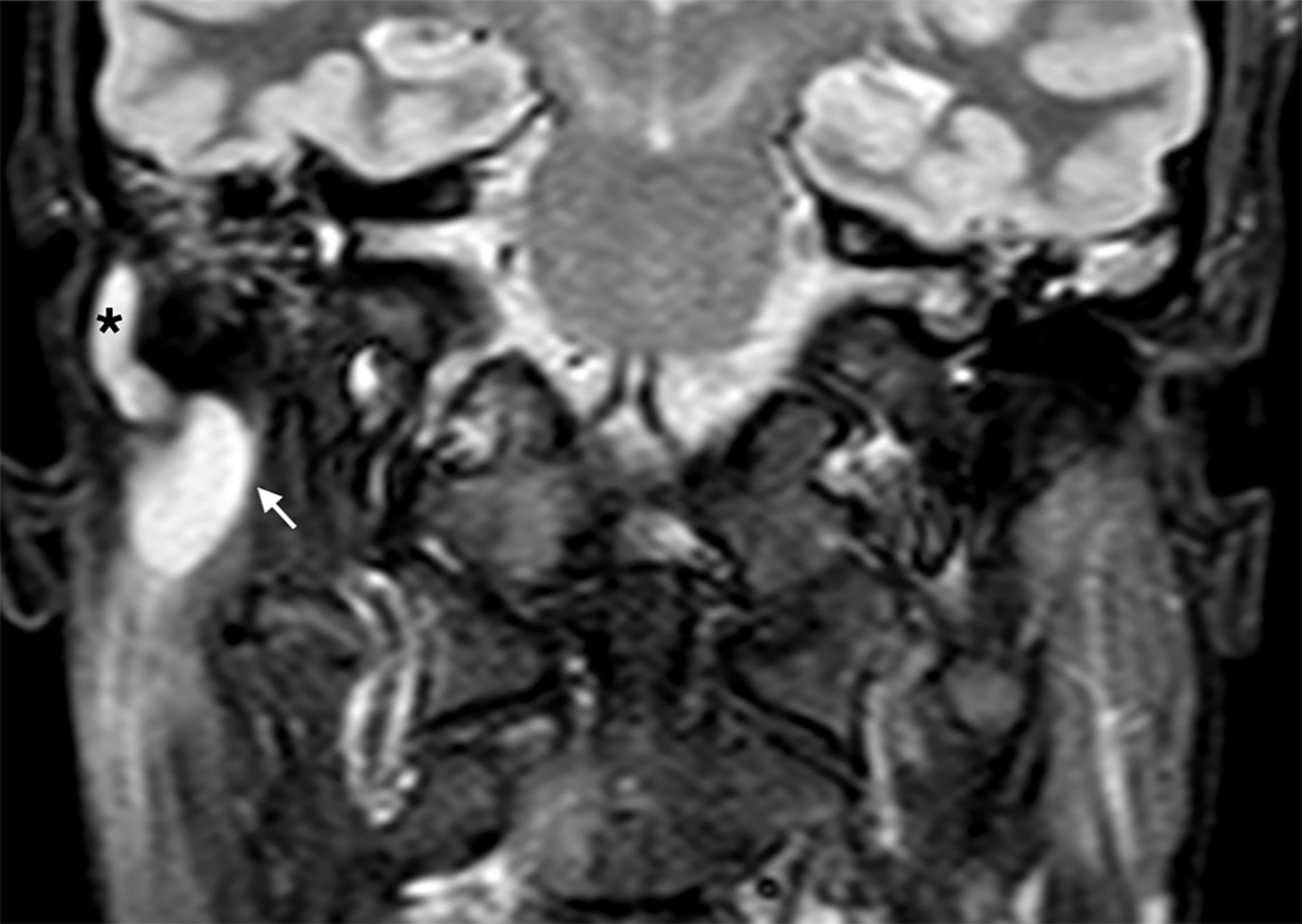
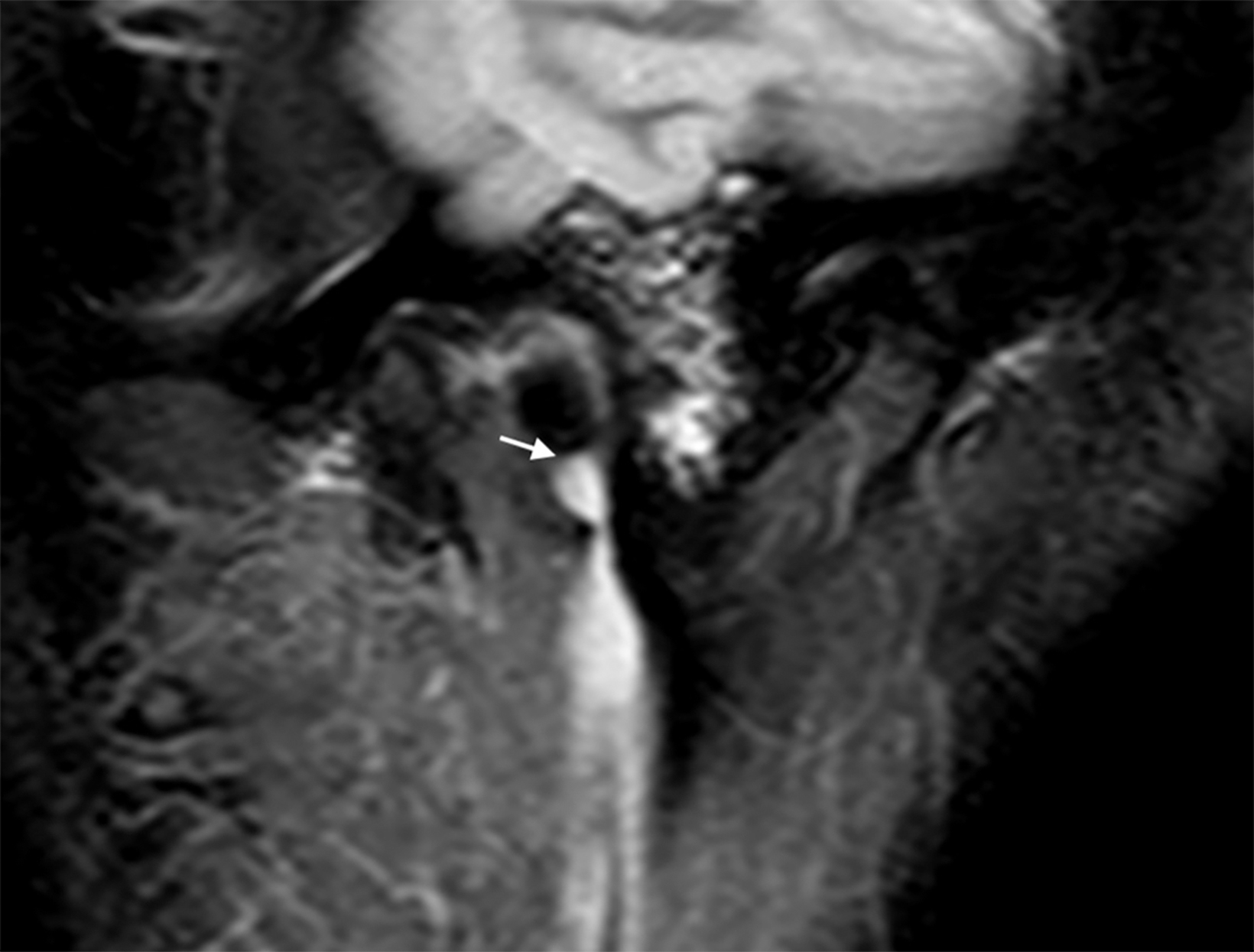
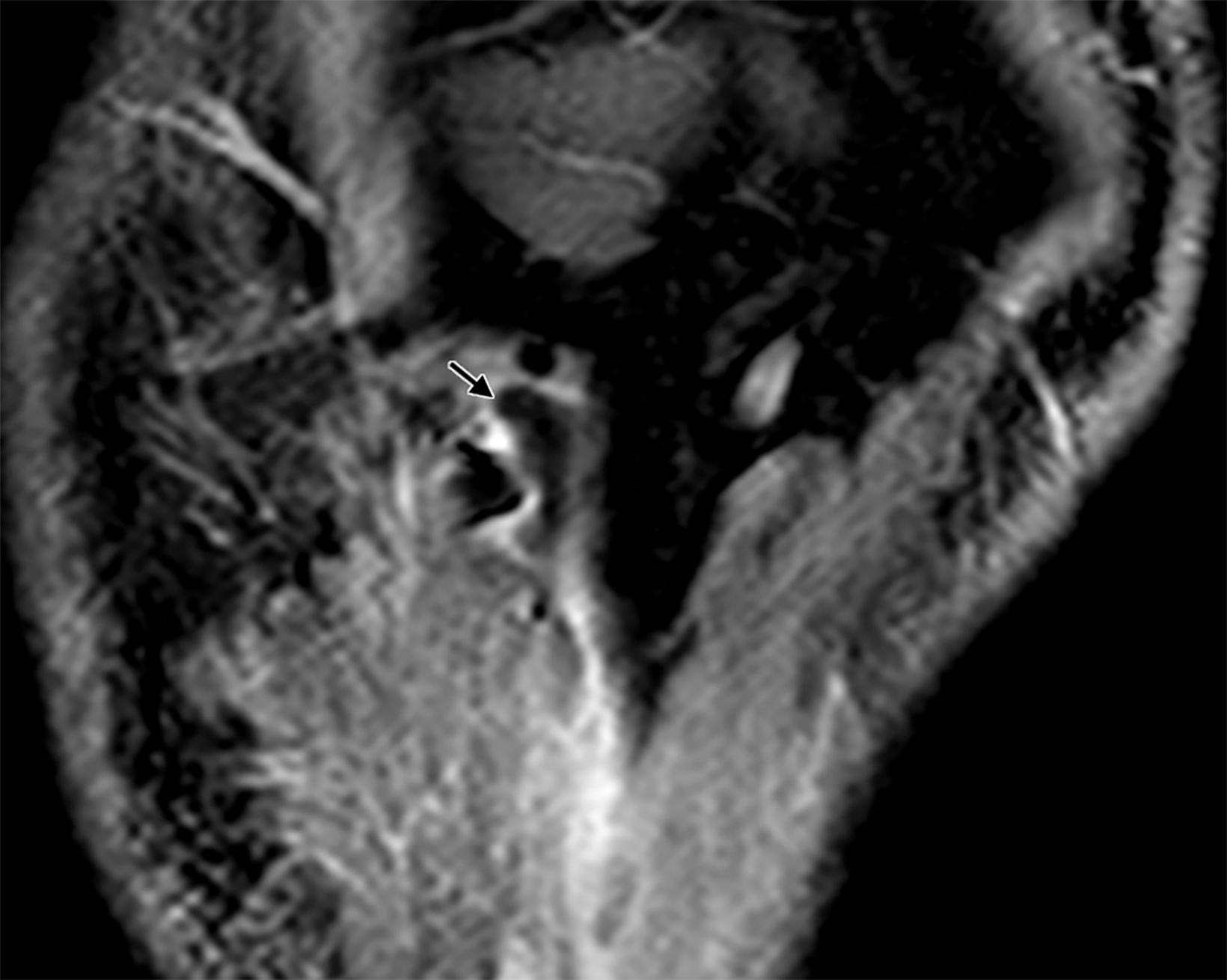
Ultrasound of the neck revealed a right, hypoechoic, homogeneous lesion of 22 × 8 ×7 mm behind the ramus of the mandible and anterior to the mastoid insertion of the sternocleidomastoid muscle. Contrast-enhanced, T2 magnetic resonance imaging (MRI) sequences of the face and neck demonstrated a hyperintense lesion of 13 × 10 × 21 mm between the right mastoid process and the posterior surface of the parotid gland, continuing with a 17 mm fistulous tract at its superior margin and running posteriorly to the posterior aspect of the cartilaginous EAC. T1 sequences with gadolinium (Figures 1,2) revealed peripheral enhancement of the lesion.
DIAGNOSIS
First branchial cleft sinus, with an EAC opening, a fistulous tract and a cystic periparotid component. The differential diagnosis includes first branchial cyst, lymphoepithelial cyst or, more rarely, localized obstructive mucocele or sialocele.
DISCUSSION
The branchial arches develop between the fourth and seventh week of gestation. During embryological development incomplete obliteration of the branchial apparatus may result in persistence of a cyst, sinus, or fistula, depending on involvement of the ectodermal cleft, mesodermal endodermal pouches, or both. A sinus is a blind-ending tract that may connect either with the skin (branchial cleft sinus) or with the pharynx (branchial pouch sinus). A fistula is a communication between two epithelialized surfaces, connecting persistent branchial cleft and pouch. In the absence of communication with either mucosa or cutaneous surface, the embryonic remnants form a cyst.1
First branchial cleft anomalies may persist anywhere in the first branchial arch, from the EAC at the level of the bony-cartilaginous junction to the submandibular triangle. The extracranial, intraparotid portion of the tract may course laterally or medially to the facial nerve.2 These account for fewer than 10% of all branchial cleft anomalies2 and for 1-4% of head and neck masses in children.1 Misdiagnosis is frequent, as the average delay between initial presentation and adequate treatment is 3.5 years.2
Depending on their clinical and histological features, first branchial cleft anomalies may be divided into two groups: type I anomalies, which are purely ectodermal in origin and represent duplication of the EAC, presenting as cystic lesions adjacent to the canal itself. Type II anomalies may present earlier in life as a cyst, sinus, or fistula of ectodermal or mesodermal origin and are located near the angle of the mandible.2,3
The clinical presentation of first arch anomalies depends on their type and location. Type I anomalies may present with purulent discharge from the EAC, or as a tumor-like mass at the mastoid level or in the posterior parotid region. Type II anomalies may present with an inflammatory mass in the parotid region or with a pit-type depression near the angle of the mandible, with possible purulent discharge during infection and related submandibular adenitis.2
On imaging, first branchial sinuses are related to the parotid gland and/or the lower margin of the pinna. The diagnosis is established if a tract directed toward the external auditory canal can be identified.4 First branchial cleft anomalies usually present on CT as cystic masses with mucoid attenuation content located superficially, within, or deep to the parotid salivary gland.
Cyst wall thickness and enhancement vary with degree of inflammation.1 Lesions frequently appear iso- or hyperintense on T1 images depending on their proteinaceous content; T2 images usually show hyperintensity1 Coronal T2 and postcontrast T1, fat-suppressed MRI may best demonstrate the tract. The cyst wall can be clearly identified on contrast-enhanced MRI.4
Resection is the standard therapy for first branchial cleft anomalies, as they usually become infected and do not regress spontaneously.1 Frequent infections can lead to formation of variable tracts with different relationships to the facial nerve. Therefore, surgical approaches differ and careful preoperative planning and protection of the facial nerve during resection are essential.3
CONCLUSION
First branchial cleft anomalies derive from the incomplete obliteration of branchial pouches during embryonic development. MRI plays a crucial role in diagnosis and differentiation of this entity from other cystic lesions of the parotid gland Surgical excision is the standard treatment, with careful surgical planning.
REFERENCES
- Adams A, Mankad K, Offiah C, Childs L. Branchial cleft anomalies: a pictorial review of embryological development and spectrum of imaging findings. Insights into Imaging. 2016; 7(1): 69-76.
- Triglia JM, Nicollas R, Ducroz V, et al.. First branchial cleft anomalies: a study of 39 cases and a review of the literature. Arch Otolaryngol.–Head and Neck Surg. 1998; 124(3): 291-295.
- Li W, Zhao L, Xu H, Li X. First branchial cleft anomalies in children: experience with 30 cases. Experim Therap Med. 2017; 14(1), 333-337.
- Curtin HD and Som PM (Eds.). Head and Neck Imaging. 2011. Mosby.
References
Citation
G C, M F, F DL.First Branchial Cleft Sinus . Appl Radiol. 2021; (6):52-53.
November 6, 2021