Endobronchial carcinoid
Images



CASE SUMMARY
A 16-year-old girl presented with a 6-month history of intermittent dry cough. For the 2 weeks prior to hospitalization, the patient had tactile fevers, right-sided chest pain, increasing wheezing, and fatigue.
IMAGING FINDINGS
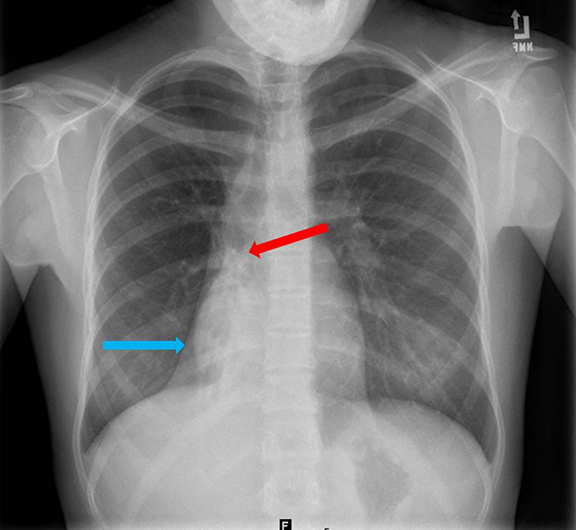
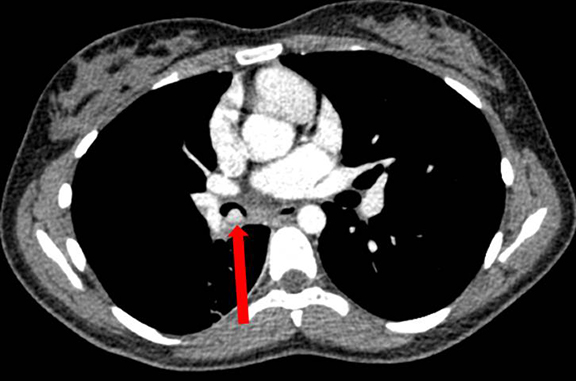
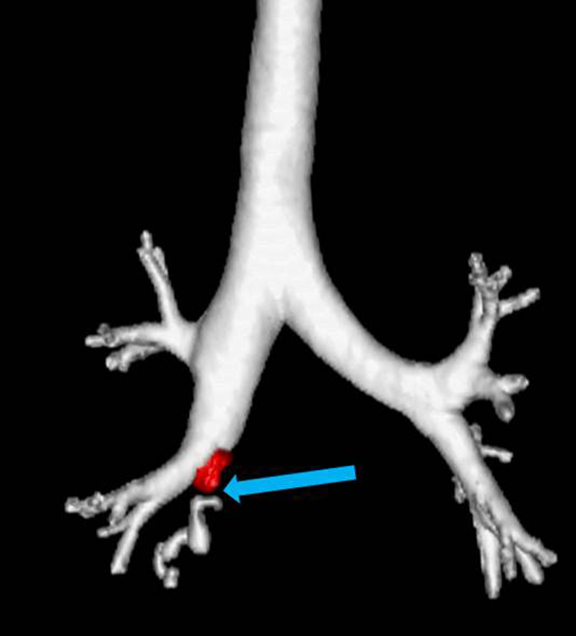
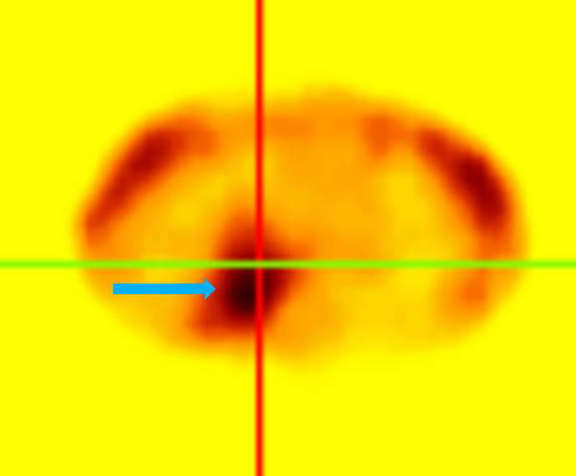
A chest radiograph (Figure 1) demonstrated right lower lobe collapse with air bronchograms. Contrast-enhanced chest CT scans (Figures 2-4) demonstrated an enhancing hypervascular endobronchial lesion within the bronchus intermedius. There was marked right lower-lobe volume loss with cylindrical bronchiectasis and mucus filling of some of the dilated bronchi. A 24-hour SPECT image from an Octreotide scan (Figure 5) showed increased radiotracer uptake within the right chest in the region of the hypervascular endobronchial lesion.
Diagnosis
Endobronchial carcinoid.
Differential Diagnoses: Carcinoid, aspirated foreign body, laryngotracheal papillomatosis, pulmonary hamartoma, and fibroepithelial polyp.
Discussion
Bronchial carcinoid tumors are neuroendocrine neoplasms that can range from low-grade typical carcinoid tumor to high-grade small cell carcinoma.1 While they are uncommon tumors, accounting for 1-5% of all pulmonary neoplasms, bronchial carcinoids are the most common primary pulmonary neoplasms in the pediatric population.1,2 Clinical presentation includes wheezing and lung atelectasis due to airway narrowing in addition to chest pain, cough and hemoptysis, but up to 25% of tumors are asymptomatic and discovered incidentally.3 Carcinoid syndrome is seen in 2% of cases and only when there is liver metastatic disease.4 Cushing syndrome is seen in about 2% when the tumor is hormonally active and produces adrenocorticotropic hormone.5
Radiologic findings depend on tumor size and location. Carcinoids are most commonly seen as a well-defined, round or oval enhancing mass located within the central airway. Approximately 80% of bronchial carcinoids are located in the main, lobar or segmental bronchi. The other 20% present as peripheral lung nodules.1 Depending on size, carcinoids can present as endobronchial nodules to large perihilar masses. If large enough to obstruct the airway, there can be peripheral lung atelectasis. Eccentric calcifications can be seen within the tumor in addition to hilar and mediastinal lymphadenopathy. Lymphadenopathy can be the result of nodal metastases or reactive hyperplasia from recurrent post obstructive pneumonia. While imaging cannot differentiate between typical and atypical bronchial carcinoids, atypical carcinoids present in older patient populations and are more likely to have nodal metastatic disease.1
Overall prognosis is good with a 10-yr survival rate of 88%. Prognosis is highly dependent on tumor grade, with atypical carcinoid 10-yr survival rate dropping to 24-52%.6,7 Treatment is surgical.
Conclusion
Endobronchial carcinoid is the most common primary pulmonary neoplasm in the pediatric population. On contrast-enhanced CT, the tumor is characteristically an enhancing mass with eccentric calcifications located within the central airway tree. It is important to look for metastatic disease as treatment is surgical resection.
References
- Jeung M, Gasser B, Gangi A et al. Bronchial carcinoid tumors of the thorax: Spectrum of radiologic findings. Radiographics. 2002; 22:351-365.
- Wang L, Wilkins E, Bode H. Bronchial carcinoid tumors in pediatric patients. Chest.1993;103:1426-1428.
- Ducrocq X, Thomas P, Massard G, et al. Operative risk and prognostic factors of typical bronchial carcinoid tumors. Ann Thoracic Surg. 1998; 65:1410–1414.
- Melmon KL, Sjoersma A, Mason DT. Distinctive clinical and therapeutic aspects of the syndrome associated with bronchial carcinoid tumors. Am J Med. 1965;39:568–581.
- Dusmet ME, McKneally MF. Pulmonary and thymic carcinoid tumors. World J Surg. 1996;20:189–195.
- Ducrocq X, Thomas P, Massard G, et al. Operative risk and prognostic factors of typical bronchial carcinoid tumors. Ann Thoracic Surg. 1998;65:1410–1414.
- Martini N, Zaman MB, Bain MS, et al. Treatment and prognosis in bronchial carcinoids involving regional lymph nodes. J Thoracic Cardiovasc Surg.1994;107:1–7.
Citation
K C, M P, SA J, AJ T, P D, R T. Endobronchial carcinoid. Appl Radiol. 2015;(5):.
May 17, 2015