Duplication cyst of the transverse colon
Images
CASE SUMMARY
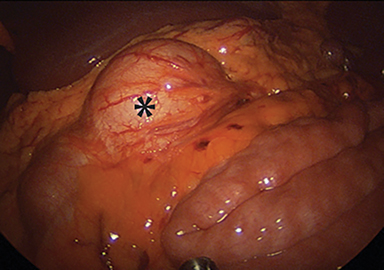
A 14-year-old girl presented with acute onset, severe, stabbing periumbilical pain awakening her from sleep. The pain progressively improved and resolved within four hours. On review of systems, she described weight loss of 19 pounds over a seven-month period associated with mild nausea and decrease of appetite. On physical examination, the patient was afebrile and vital signs were normal. However, she was tender to deep palpation in the periumbilical area. Laboratory values were normal; specifically, WBC count was 6,500/mCL and ESR was 5 mm/hour. The patient underwent colonoscopy and upper endoscopy. Upper endoscopy revealed gastritis, but was otherwise normal. On colonoscopy, a partially obstructing noncircumferential mass was located at the splenic flexure. Biopsy revealed gastric mucosa lining the mass, and diagnosis of presumed colonic duplication cyst was made. The mass was laparoscopically resected with primary reanastomosis of the distal transverse colon (Figure 1).
IMAGING FINDINGS
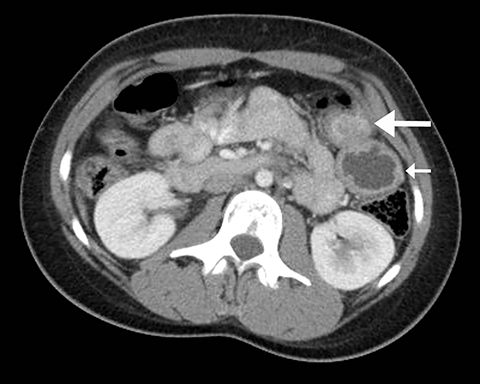
CT with oral and intravenous contrast was performed. A 2.9 × 2.4 × 2.1 cm solid enhancing mass in the distal transverse colon was appreciated, with a centrally hypodense thick walled exophytic component measuring 4.0 × 3.4 × 3.3 cm (Figure 2). No adjacent fat stranding was noted, nor any additional signs of acute inflammation, such as adenopathy or free fluid.
DIAGNOSIS
Colonic duplication cyst. Other less likely differential considerations include primary colonic malignancy (adenocarcinoma), atypical gastrointestinal stromal tumor (GIST), intestinal lymphoma, or loculated perforation.
DISCUSSION
Duplications of the gastrointestinal (GI) tract are rare congenital anomalies found anywhere along the GI tract, from mouth to anus. Structurally, they can be cystic or tubular and contain well-developed smooth muscle lined with alimentary tract mucosa.1,2 Age of presentation typically ranges from the neonatal period to the second decade, although they can present in adulthood.1,2 In a review by Macpherson, four major studies with a total of 281 enteric duplications were analyzed. In this meta-analysis, duplications were most commonly found in the ileum (33%) followed by the esophagus (20%), colon (13%), jejunum (10%), stomach (7%) and duodenum (5%).2 Spherical cysts are the most common basic structure constituting approximately 80% of duplications; these typically do not communicate with the adjacent lumen. The mucosal lining does not always correlate with the adjacent GI tissue. Ectopic gastric and pancreatic mucosa are most often symptomatic. Ectopic gastric mucosa is most typically found in esophageal, small bowel or thoracoabdominal duplications, and ectopic pancreatic mucosa is most common to gastric duplications.2
More than half of all colonic duplications are cystic and have very different attributes from the tubular colorectal duplications, as they do not communicate with the adjacent lumen. Notable also is the lining of the mucosa in this case, as gastric mucosa is only found in approximately 2% of all colonic duplications.2
Consideration in selection of imaging modality is dependent on the signs, symptoms and timing of presentation. Duplications most commonly present with pain or symptoms related to obstruction or hemorrhage. Ultrasound is frequently used, and is the most common imaging modality used in evaluation of small bowel duplications.3 Characteristic sonographic findings include a well described double wall appearance consisting of an inner hyperechoic layer representing the mucosa and submucosa, and an outer hypoechoic layer with sharper edges correlating to the muscularis propria.4,5 However, false positives have been reported in cases of Meckel’s diverticulum and ovarian torsion. The five layer structure of bowel is a more specific finding but is less frequently seen.4 Peristalsis is another sonographic feature which has been described as helpful in distinguishing enteric duplication from other cystic abdominal masses.6
Contrast study performed under fluoroscopy is another common modality used in evaluation of suspected duplication. For example, studies such as upper GI with small bowel follow-through or barium enema can demonstrate either an extrinsic mass or presence of contrast in an adjacent lumen.3,7
While CT and MRI can provide useful information in equivocal cases, they are less frequently used, given radiation dose with CT and need for sedation with MRI.3 In the present case, however, CT was utilized given the acuity of presentation. On CT, duplication cysts have been characterized as fluid filled structures with thinly enhancing walls in or adjacent to the gut wall.7 A similar appearance was noted on the current exam. Nodular calcifications have been described, though not appreciated in the current case.8 On MRI, duplication cysts appear heterogeneous on T1-weighted sequences, while uniformly hyperintense on T2-weighted sequences.7
Finally, nuclear medicine evaluation can be helpful in duplications containing gastric mucosa as these will demonstrate uptake on technetium-99m pertechnetate scintigraphy.3
CONCLUSION
In summary, we have described a case of a duplication cyst in the transverse colon presenting with acute abdominal pain. Though rare, colonic duplication cysts can be considered in differential diagnosis of a cystic abdominal mass in a pediatric patient, as over half of all duplication cysts are cystic.
REFERENCES
- Gross RE, Holcomb GW, Jr., Farber S. Duplications of the alimentary tract. Pediatrics. 1952;9:448-468.
- Macpherson RI. Gastrointestinal tract duplications: clinical, pathologic, etiologic, and radiologic considerations. Radiographics: a review publication of the Radiological Society of North America, Inc. 1993;13:1063-1080.
- Hur J, Yoon CS, Kim MJ, Kim OH. Imaging features of gastrointestinal tract duplications in infants and children: from oesophagus to rectum. Pediatric radiology. 2007;37:691-699.
- Cheng G, Soboleski D, Daneman A, Poenaru D, Hurlbut D. Sonographic pitfalls in the diagnosis of enteric duplication cysts. AJR American Journal of Roentgenology. 2005;184:521-525.
- Barr LL, Hayden CK, Jr., Stansberry SD, Swischuk LE. Enteric duplication cysts in children: are their ultrasonographic wall characteristics diagnostic? Pediatric Radiology. 1990;20:326-328.
- Spottswood SE. Peristalsis in duplication cyst: a new diagnostic sonographic finding. Pediatric Radiology. 1994;24:344-345.
- Berrocal T, Lamas M, Gutieerrez J, Torres I, Prieto C, del Hoyo ML. Congenital anomalies of the small intestine, colon, and rectum. Radiographics: a review publication of the Radiological Society of North America, Inc. 1999;19:1219-1236.
- Dutheil-Doco A, Ducou Le Pointe H, Larroquet M, Ben Lagha N, Montagne J. A case of perforated cystic duplication of the transverse colon. Pediatric Radiology. 1998;28:20-22.
Citation
C S, N S, JY C.Duplication cyst of the transverse colon. Appl Radiol. 2017; (9):36-37.
September 4, 2017