Dorsal Thoracic Arachnoid Web and Spinal Cord Compression
Images




CASE SUMMARY
A 64-year-old presented with a 3-year history of progressive back pain, lower limb weakness, and unstable gait. They experienced no bowel or bladder difficulty and denied any history of prior trauma, spinal surgery, or spinal inflammation. Physical examination revealed lower limb weakness with spasticity.
IMAGING FINDINGS
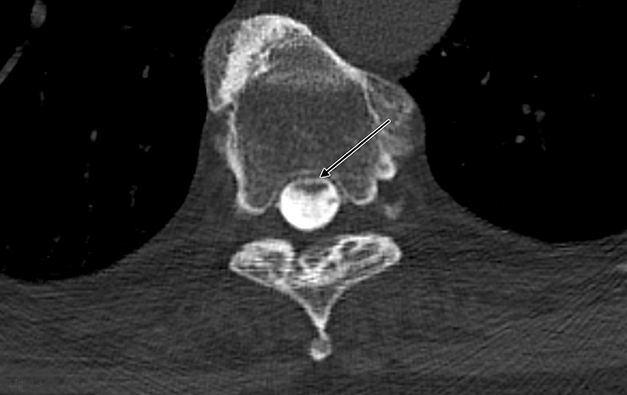
Magnetic resonance imaging (MRI) demonstrated a focal dorsal indentation of the thoracic spinal cord at the T6 level, with associated compression and deformity of the cord, which was displaced anteriorly (Figure 1). Extensive spinal cord signal abnormality was present below the level of the indentation, extending to the T8 level. No abnormal contrast enhancement was present (Figure 2). CT myelography showed the “upside down scalpel sign,” with the characteristic focal indentation of the dorsal thoracic spinal cord, widening of the dorsal cerebrospinal fluid (CSF) space, and spinal cord expansion below the level of the dorsal indentation. No filling defects were demonstrated on the myelogram to indicate the alternative diagnoses of arachnoid cyst or ventral cord herniation. Myelography through the level of the dorsal indentation demonstrated a remaining thin CSF space between the anterior cord and the ventral thecal sac.
DIAGNOSIS
Dorsal thoracic arachnoid web with spinal cord compression. Differential diagnosis includes ventral spinal cord herniation and dorsal arachnoid cyst.
DISCUSSION
Spinal arachnoid webs represent intradural, extramedullary bands of arachnoid tissue that extend to the pial surface of the spinal cord. They are an uncommon entity that typically occurs in the upper thoracic spine, producing a focal indentation on the dorsal spinal cord.1
There is lack of consensus on the terminology describing arachnoid webs, and their differentiation from other forms of arachnopathies, such as arachnoid adhesions, arachnoid scarring, and arachnoiditis. 1 Arachnoid webs have been known to develop after focal inflammation or trauma in the spine. 1 However, there have also been reports of non-traumatic arachnoid webs of unknown etiology, leading to consideration of congenital arachnoid webs, associated with a thickened ligamentum flavum.2 It has been proposed that arachnoid webs arise from the process of formation or collapse of arachnoid cysts. 1,3 Arachnoid webs can disrupt the normal craniocaudal flow of CSF, leading to focal compression of the spinal cord and/or syringomyelia. 4,5
Owing to their thin structure, spinal arachnoid webs are not readily visualized on routine imaging. 6 Instead, they produce a characteristic dorsal indentation of the cord on MRI and CT myelography, described as the “scalpel sign,” with the “blade” pointing posteriorly. 4,7
Anterior displacement of the spinal cord, an abrupt change in spinal cord caliber, or evidence of adjacent syringomyelia are other important secondary imaging signs. 4 The topological relationship of the arachnoid web to the syrinx is variable. Klekamp reported a rostrally located syrinx in 47% of cases, caudally located syrinx in 24% of cases, and bilocalized syrinx in 29% of cases.8
MRI CSF flow studies have also been advantageous in providing an early diagnosis of arachnoid webs by demonstrating disrupted CSF flow dynamics.2,9 Arachnoid webs can be accurately localized by assessing the site of CSF flow blockage.2
Spinal arachnoid webs can be definitively diagnosed with intraoperative ultrasound, where they resemble membrane-like structures in the dorsal subarachnoid space, moving in sync with the cardiac cycle.1,2
Surgical opening of the dura allows direct visualization of the arachnoid webs and provides an opportunity to restore the normal CSF pathway. Options for management of a symptomatic arachnoid web include marsupialization, fenestration, or laminectomy with exploration of the intradural space and subsequent resection of the arachnoid web.1,10,11 Postoperative MRI CSF flow study should demonstrate improved flow dynamics.
Failure to consider arachnoid web as a diagnosis preoperatively increases the risk of future myelopathy, and diagnosis prior to development of spinal cord signal abnormality and syringomyelia reduces morbidity. 6,9
Differential diagnoses are ventral spinal cord herniation and dorsal arachnoid cyst. In ventral spinal cord herniation, there is deformity of the ventral surface of the spinal cord as it protrudes through a ventral dural defect, and no space between the spinal cord and ventral thecal sac. Arachnoid cysts can be identified, particularly on thin-section volumetric MR by their marginated walls, and they produce a relatively smooth scalloping on the spinal cord surface.1,12 An intraspinal filling defect with delayed filling of the arachnoid cyst are also present on myelography. In our case, the patient underwent surgical decompression with symptomatic improvement.
CONCLUSION
Spinal arachnoid webs demonstrate relatively typical imaging features, with characteristic focal indentation of the dorsal spinal cord and widening of the dorsal CSF space on MR and CT myelography. Their association with syringomyelia and spinal cord compression can result in significant patient morbidity, and identification of the described imaging features facilitates early diagnosis and prompt surgical treatment to prevent progressive myelopathy.
REFERENCES
- Zhang D, Papavassiliou E. Spinal intradural arachnoid webs causing spinal cord compression with inconclusive preoperative imaging: A Report of 3 cases and a review of the literature. World Neurosurgery. 2017 Mar; 99: 251–8.
- Chang HS, Nagai A, Oya S, et al. Dorsal spinal arachnoid web diagnosed with the quantitative measurement of cerebrospinal fluid flow on magnetic resonance imaging. J Neurosurg Spine. 2014; 20: 227-33.
- Paramore CG. Dorsal arachnoid web with spinal cord compression: variant of an arachnoid cyst? Report of two cases. J Neurosurg. 2000; 93: 287-290.
- Reardon MA, Raghavan P, Carpenter-Bailey K, Mukherjee S, Smith JS, Matsumoto JA, et al. Dorsal thoracic arachnoid web and the “scalpel sign”: a distinct clinical-radiologic entity. Am J Neuroradiol. 2013; 34: 1104-1110.
- Hubbard ME, Hunt MA, Jones KE, Polly DW. Thoracic spinal cord impingement by an arachnoid web at the level of a hemivertebra: case report. J Neurosurg Spine. American Association of Neurological Surgeons. 2017 Dec; 27(6): 638–42.
- Sayal PP, Zafar A, Carroll TA. Syringomyelia secondary to “occult” dorsal arachnoid webs: Report of two cases with review of literature. Journal of Craniovertebral Junction & Spine. 2016; 7(2): 101-104.
- Aiyer R, Voutsinas L, El-Sherif Y. An overview of arachnoid webs. The J Neurol Neuromed. 2016; 1(6): 66-68.
- Klekamp J, Batzdorf U, Samii M, Bothe HW. Treatment of syringomyelia associated with arachnoid scarring caused by arachnoiditis or trauma. J Neurosurg. 1997; 86: 233–240.
- Mauer UM, Freude G, Danz B, Kunz U. Cardiac-gated phase—contrast magnetic resonance imaging of cerebrospinal fluid flow in the diagnosis of idiopathic syringomyelia. Neurosurgery. 2008; 63 (6): 1139–1144.
- Gottschalk A, Schmitz B, Mauer UM, Bornstedt A, Steinhoff S, Danz B, et al. Dynamic visualization of arachnoid adhesions in a patient with idiopathic syringomyelia using high-resolution cine magnetic resonance imaging at 3T. J Magn Reson Imaging. 2010; 32: 218–222.
- Petridis AK, Doukas A, Barth H, Mehdorn HM. Spinal cord compression caused by idiopathic intradural arachnoid cysts of the spine: review of the literature and illustrated case. Eur Spine J. 2010; 19: S124-S129.
- Wang MY, Levi AD, Green BA. Intradural spinal arachnoid cysts in adults. Surg Neurol. 2003; 60:49-55.
Citation
TY S, K B, WA M. Dorsal Thoracic Arachnoid Web and Spinal Cord Compression. Appl Radiol. 2020; (5):52-54.
September 1, 2020