Calcaneal bone osteomyelitis
Images

Prepared by Walter Silbert, MD and Maroun Karam, MD, Department of Radiology, Albany Medical College, Albany, NY.
CASE SUMMARY
A 51-year-old white man with a medical history significant for Type I diabetes mellitus and peripheral vascular disease necessitating multiple prior distal amputations presented with increasing right foot pain. He reported no recent trauma or corticosteroid therapy. Physical examination revealed prior transmetatarsal amputation and a large nonhealing ulcer that penetrated deeply to the lateral aspect of the ankle. In addition, erythema, warmth, and edema of the leg and foot were noted, leading to a strong clinical suspicion of osteomyelitis.
DIAGNOSIS
Calcaneal bone osteomyelitis
IMAGING FINDINGS
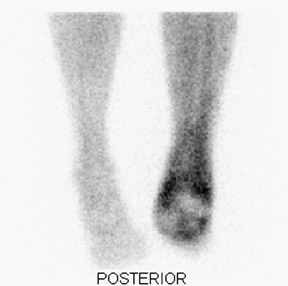
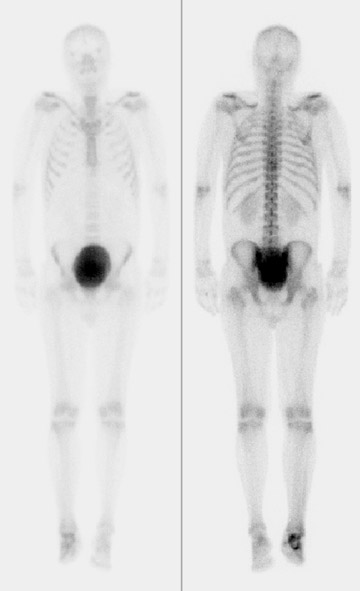
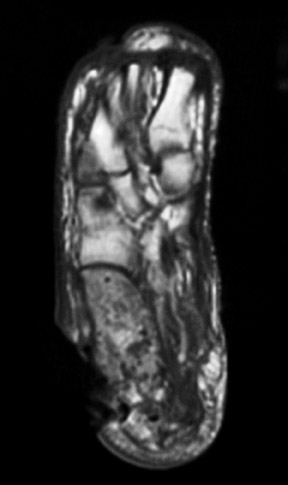
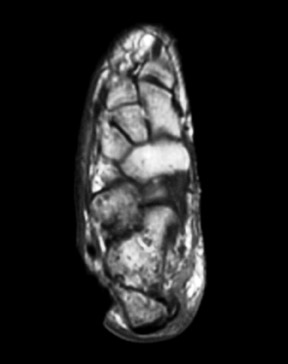
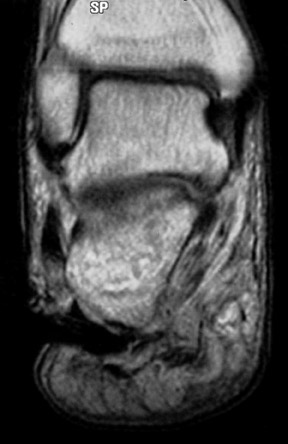
Radiographic examination revealed a mildly dis-placed fracture of the calcaneal tuberosity (Figure 1). Focal bone lysis and periosteal reaction typical of osteomyelitis were not appreciated. However, they may not be detected for 7 to 14 days. Given the strong clinical suspicion of osteomyelitis, a technetium-99m methylene disphosphonate three-phase bone scan was requested, which revealed increased blood flow and soft-tissue uptake in the right lower extremity and a photopenic focus in the region of the calcaneal tuberosity on delayed imaging (Figure 2). A diagnosis of lower extremity cellulitis and aseptic necrosis of the calcaneus was suggested. Subsequent magnetic resonance imaging (MRI) revealed mild diffuse marrow signal abnormality within the posterior calcaneal fracture fragment. However, there was no localized area of intense marrow infiltration along the lateral aspect of the calcaneus abutting the nonhealing ulcer to support the diagnosis of osteomyelitis (Figure 3A). In addition, anterior to the fracture line, a serpiginous region of low signal intensity was seen on both T1- and T2-weighted images, corre-sponding to the photopenic area on the bone scan, a specific characteristic of a bone infarct (Figures 3B and 3C). A lower extremity angiogram revealed occluded anterior and posterior tibial arteries with reconstitution of the dorsal and plantar arches via collaterals.
DISCUSSION
Bone infarction is also known as osteonecrosis. 1,2 All forms of osteonecrosis result from ischemic death of cellular constituents of bone and marrow. The mechanisms that produce ischemia include mechanical vascular interruption, corticosteroids, thrombosis and embolism, vessel injury due to vasculitis or radiation injury, increased intraosseous pressure with vascular compromise, and venous hypertension. Usual causes include trauma, steroids, sickle cell anemia, dysbaric causes, systemic lupus erythematosis, Gaucher's disease, alcoholism, and pancreatitis. The pathologic features of osteonecrosis are the same regardless of the cause. 6
A localized cold lesion on bone scan is nonspecific for bone infarction and may also be seen with early osteomyelitis and marrow involvement by primary or metastatic tumor. The earliest MRI appearance of bone infarction, marrow edema, is also nonspecific. However, there is rapid progression to a distinctive, well-defined pattern that allows a specific diagnosis to be made. The characteristic pattern is a low signal intensity serpentine rim at the interface of living and dead bone on both T1- and T2-weighted images. This corresponds to the margin of advancing new bone and granulation tissue histologically. The early and specific diagnosis of bone infarction by MRI allows early appropriate intervention to reduce the risk of potential complications, including bone collapse and secondary degenerative joint disease. 7
Given the finding of perfusion of the dorsal and plantar arches via collaterals on angiography, and a negative history for steroid treatment, the bone infarct in this case may be a consequence of spontaneous calcaneus fracture with resulting mechanical vascular interruption. Spontaneous fracture in this patient is not surprising. In addition to bone resorption, resulting from hyperemia secondary to the adjacent nonhealing ulcer, diabetes mellitus results in decreased bone mineralization via multiple pathological processes. Diabetes alone is known to be associated with decreased bone density before other complications become clinically evident. Neuropathic changes may also contribute to bone loss in diabetic patients through altered weight bearing. In addition, nephropathy and uremia are associated with abnormal or decreased bone mineralization. 5
Diabetes mellitus, peripheral vascular disease, and hyperemia secondary to soft-tissue infection predisposes to calcaneal insufficiency fractures that may disrupt intraosseous vasculature and result in bone infarction. To the best of our knowledge, few cases of calcaneal bone infarction detected by bone scanning are reported in the literature. 4
CONCLUSION
Although nonspecific, a cold defect on a bone scan is suggestive of bone infarction in this clinical setting. The diagnosis was confirmed in this case by MRI. Early and accurate diagnosis of bone infarction facilitates appropriate management, reducing the risk of bone collapse and secondary degenerative disease.
Products used
- Diacam dual-head gamma camera (Siemens Medical Solutions, Hoffman Estates, IL)
- Signa 1.5TMRI scanner (GE Healthcare, Waukesha, WI)
- 25 mCi of Tc-99m MDP