Applied Radiology Focus: Three-dimensional image rendering for CT
Images






Helical, or spiral, computed tomography (CT) is, by its very nature, a volumetric acquisition method. Recent advances in both hardware and software capabilities are now bringing the full power of this volumetric data acquisition to clinical practice in the form of real-time, interactive 3-dimensional (3D) imaging. "Traditionally, CT provided a fairly slow acquisition of axial slice information," said Carter Newton, MD, Consultant on CT Imaging, South Carolina Heart Center, Columbia, SC. "In the early days of CT, radiologists were able to stack these axial images together, albeit sometimes a little bit awkwardly, and get volume approximations that were assembled over time. What spiral CT has enabled us to do, particularly as the technology has accelerated, is to acquire entire volumes of information and assemble these volumes on a computer. Once the volumes are on the computer, we can use the power of the processing and the power of the software to render the images from new perspectives so that all elements of the volume can be viewed and understood in their natural anatomic relationships."
Development of 3D rendering for CT
"The use of 3D with CT imaging started roughly 25 years ago at the Mayo Clinic (Rochester, MN)," said John Rumberger, MD, PhD, Professor of Medicine, Ohio State University, and Medical Director of HealthWISE Wellness Diagnostic Center, Columbus, OH. "At that time, however, it was very labor-intensive to make 3D images from a CT scan. The more recent improvements in computer technology have allowed us to go from a system that required an hour or more to make a single reasonable image to real-time 3D imaging with continuous one-on-one interaction with the volume dataset."
"The software available now is so powerful that it can handle very large volumes of data and postprocess it very quickly," agreed Michael Poon, MD, Director of Cardiovascular Medicine and Integrated Medical Program, Cabrini Medical Center, New York, NY. "In the past, this was not possible because the computer and the software were not capable of performing these functions quickly."
How 3D imaging works
"With CT, one acquires volumetric datasets one slice at a time or, as is the case with the new multirow detector CTs (MDCTs), in multiple slices at a time," said J. Anthony Seibert, PhD, Professor of Radiology, University of California, Davis, Imaging Research Center, Sacremento, CA. "What the 3D capability allows one to do then is to become unhindered by the need to look at just the axial slices sequentially. In essence, it provides a look into the volumetric datasets by reformatting the information."
"With the evolution of MDCT, the acquired data have more isotropic resolution," explained Geoffrey D. Rubin, MD, Chief of Cardiovascular Imaging and Associate Professor, Stanford University School of Medicine, Stanford, CA. "The section's thickness now approaches the resolution in plane of the individual pixel. So what you end up having when you stack all cross sections together is a volume of data that has almost the same resolution regardless of what direction you look at it."
Once acquired, the volumetric datasets can then be reconstructed in a variety of formats. "One can do what is known as multiplanar reconstruction to achieve views from different projections such as the sagittal, coronal, or any oblique plane," noted Seibert. "Or, one can take the dataset and can average slices to reduce noise or improve the signal-to-noise ratio. With maximum intensity projection (MIP), one is able to take a different view of information contained in thick slices of information and display only the brightest intensity components within that particular slab of information, which is useful when looking for high-density material such as calcifications or iodinated vasculature."
"With 3D imaging," added Jonathan Hartman, MD, Assistant Professor of Radiology, Director of Neurointerventional Radiology, University of California, Davis, Sacramento, CA, "you are taking multiple thin-section, usually axial, images and reconstructing them into a 3D image. By doing that, you can take that dataset and manipulate it, rotate it into different views, and generally get a better understanding of the relationship of one structure to another or of what a structure looks like along its length as opposed to just on a single transaxial image."
"With full 3D volume rendering of the dataset, one is able to, by appropriate shading and coloring and perspective, produce a 3D volume of the information that is truly useful in surgical planning and in identifying critical areas for avoidance or targeting," said Seibert.
Currently available products
"The algorithms used to reconstruct CT images into 3D are mainly in the public domain, so there are tremendous similarities among the products offered by the various vendors," said Rumberger. But there are some differences. "Some vendors use different processing tools. Others change the computers by increasing the RAM [random access memory]. One company has a proprietary parallel processor accelerator board to speed up the ability to make the images. But, in general, the basic computer algorithms are fairly well standardized within the industry; it's just a matter of how they are applied within any given system."
The most significant difference among products relates to where the software is located. Some CT scanners are available with 3D software pre-installed, essentially making the CT workstation the 3D workstation as well. Some vendors provide dedicated stand-alone 3D workstations, while others sell thin-client server software that can be attached to the picture archiving and communication system (PACS).
"We have both systems here," said Daniel Nguyen, MD, Director of Neuroradiology and Director of 3D Imaging and Surgical Planning Services, Georgetown University Hospital, Washington, DC. "We have a dedicated 3D workstation that has all the power of the different tools that current workstations have, but we also have a system that has easier access to the datasets and allows the user to perform 3D from the PACS workstation without having to move to a dedicated workstation. Choosing which system to use depends on the case," he continued. "If the case is simple and requires no additional 3D views, then we use the thin-client server model to view it. If it's very difficult and we need different tools, then we do it at the dedicated workstation."
"One of the nice attributes of the way in which we have implemented much of our 3D imaging capabilities is the use of the third-party add-on with our PACS," said Seibert. "The ability to seamlessly interact with a volumetric dataset and then go into the 3D rendering software is a real value for the radiologist who previously had to get up and go to another workstation. Now, with a single right mouse click, one is able to launch the application."
Incorporating 3D into clinical workflow
Image reconstruction
At some institutions, the 3D reconstruction is handled, at least in part, by the CT technologists, but in many cases, it is the radiologists themselves who perform the postprocessing.
"This is something that will vary from institution to institution, even from person to person," said Hartman. "A lot of places use technologists. CT technologists are at the forefront of reconstruction work. It's helpful, but they do not always have the same appreciation for what the specific view or the specific pathology is, so they may miss something. That can be a pitfall."
"At our institution, we have two parallel models for 3D postprocessing," said Rubin. "We have a 3D laboratory that was established in 1996 that is focused on processing critical data for both CT and magnetic resonance imaging (MRI). It is staffed by 5 full-time technologists, who are either CT or MRI technologists, and a support staff. They process up to 700 clinical cases per month. They mainly create protocol visualizations, but they also perform a lot of quantitative work. They will measure tissue volumes and dimensions of structures, such as blood vessels and parenchymal organs, that are not easily measured using standard transverse sections."
Georgetown University Hospital also uses a dual process. "The technologists do standard orthogonal views, and we have a 3D thin-client central server system that allows radiologists to quickly access the dataset, reconstruct it, and view it to make better diagnoses," explained Nguyen. "Sometimes certain standard views do not portray the pathology as well, so you have to use your expertise, and that's where the radiologists make some adjustments to the standard views."
"In cardiology, we do the reconstruction," said Poon. "The technologists often scan the patients and we take the reconstructions. At some centers, the technologists do a lot of the trimming; they get rid of the bone or structures that are not germane to the diagnosis."
"The reason for technologists to do it, theoretically, is to save time and present the radiologist with certain views," added Charles Truwit, MD, Chief of Radiology, Hennepin County Medical Center and The Margaret and H.O. Peterson Chair in Neuroradiology, University of Minnesota, Minneapolis, MN. "There are those among the radiologists here at my institution who still are not, perhaps, as gifted as they could be, and being gifted comes from practice. But most of us find that it is far faster for us to operate the system ourselves and it's of little benefit to have somebody prepare the work a priori."
Reviewing 3D images
When reviewing 3D images, it is important to remember that this technology is an adjunct to axial imaging-it does not replace it. "You can get most of the information from the reconstructed image but not all of it," said Hartman.
"In my practice, I look at the cardiac vessels predominantly," explained Poon. "When I load the images, I always go to the 3D images first because it gives me the same type of view that I am used to seeing from X-ray angiography. I use the workstation to do the postprocessing to create the 3D image of the coronary, and that allows me to look for the orientation of the vessels and any gross evidence of pathology. From there, I hone in on specific lesions. I then go to the 2-dimensional (2D) images to look at the specific area where the pathology is located to determine what kind of disease process is present and how severe the stenosis is."
"The best images that you are ever going to have are the images that you acquire directly from the scanner," added Rumberger. "Anything else is really postprocessing, and when you decide to limit the views by various tools that allow you to possibly enhance various features, you lose information. So, as with any postprocessing, you have to be sure that the information lost is not vital to your interpretation."
"There are times when I may be looking at a noninvasive coronary arteriogram done by CT and I see a specific area and I think that it is normal, but then I make a 3D picture and because of the parameters I chose on the 3D picture, all of the sudden it will look like there is a blockage," he continued. "I will realize that I have in a sense created it by selecting various material properties, properties of the densities. I then have to go back and fix them. It is often challenging with 3D. When you see something with 3D, especially if you are looking for vessel blockages, the next step is to try to make it go away by varying the processing. If you try everything and there is still a blockage, then that's your answer."
"If one is not familiar with the methods of creating 3D images, there is a risk of misinterpreting them," agreed Rubin. "So, as with any new technique in radiology, it is not sufficient to look at an image and assume that you know how to completely interpret it. Radiologists must interpret 3D images in association with cross-sectional images and with an understanding of volume-rendering parameters, techniques, and pitfalls."
Clinical applications
"There are certain types of CT applications for which 3D seems to be more optimally suited or at least used more frequently right now," said Rubin. "Probably the greatest use is in the vascular system, CT angiography (CTA) specifically. Virtually all CTAs are performed and interpreted with 3D analysis. One occasional exception might be the search for a pulmonary embolism, but otherwise, being able to create a 3D map of complex vascular structures and their relationship to adjacent structures is a real advantage over looking at cross sections."
"Other areas where 3D is used is in orthopedic imaging, particularly skeletal lesions and complex fractures, such as those in the thalamus or the tibial plateau, as well as the bones of the foot, rib, elbow, and many joints," he continued. "3D is also used to look at parenchymal lesions and lung nodules. It's also used to evaluate the pancreas and to look at pancreatic masses and their relationship to adjacent structures. I've also seen a great increase in the use of 3D in the genitourinary system, particularly the kidneys with the evolution of the new technique of CT urography."
In his vascular imaging practice, Hartman noted that 3D imaging is helpful in detecting aneurysms. "It's very useful for looking at the blood vessels when you are searching for an aneurysm or defining the anatomy of the aneurysm and the relationship of the blood vessels and the skull base," he stated. "The other area in which I think it has been helpful, especially for the surgeons, is for fractures. We have a pretty large volume of trauma patients here, and we are routinely doing more reconstructions for the craniofacial surgeons, the orthopedic surgeons, and the neurosurgeons. This gives the clinicians a better appreciation of how the bone fragments are relating to each other. The 3D images give them an almost life-like view of what is going on."
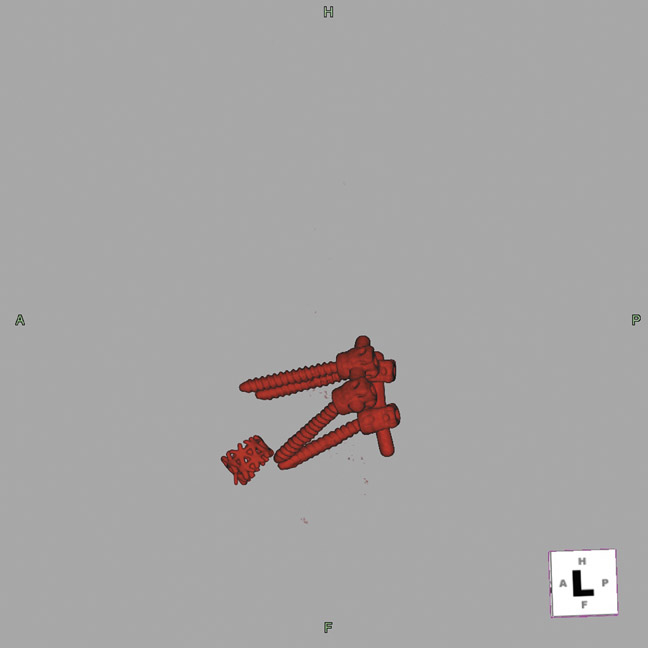
Nguyen noted that 3D is also useful in his neuroradiology practice. "We always use 3D," he explained, "because the traditional axial images are not sufficient to diagnose pathology. I always use it in my angiograms and in my spine work. I like the ability to look at the spine in a 3D format and to critique its alignment, and to evaluate surgical device placement (Figure 1). In a 2D image, it is hard to conceptualize, so I use 3D technology in roughly 90% of my work."
"This is an exciting area, and there is a lot of potential utility in the use of 3D image processing," added Poon. "Every time we look at it, another indication pops up, such as using CT in the emergency department to rule out chest pain. Chest pain is one of the most difficult diagnoses to work-up because of the potential liability. Chest pain is very broad; it could be a dissection, it could be a pulmonary embolism, it could be coronary artery disease. With this kind of 3D CT imaging, you can rule out many of the disastrous possibilities with one scan. Using the advanced multislice scanner and the 3D reconstruction technology, we can quickly get a bird's-eye view of the entire thorax."
Among all of the 3D imaging studies currently used in CT practice, the two that are most widely used are CT colonography, also known as "virtual colonoscopy," and CTA.
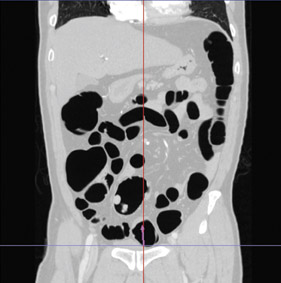
"Virtual colonoscopy using CT is a 3D method of analysis," explained Poon. "It is very much like a colonoscopy." With this procedure, the patient undergoes the same bowel preparation procedure but, instead of undergoing traditional colonoscopy, they undergo CT scanning (Figure 2).
"Virtual colonoscopy is getting better and better," said Rumberger. "We're learning how to do the preparations properly. We're learning how to process the images. All 3D imaging requires the radiologist to go back to school a little bit. I thought it was intuitive but it's not. It's a learning process. You really need to understand how those images were created before you can comprehend how to use them."
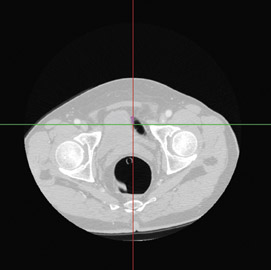
"Cardiac angiography (Figure 3) with volume CT scanners is also now a reality, and, in fact, because of the 3D rendering capabilities, one is able to make a better differential diagnosis and have a much safer procedure relative to putting a catheter internal to the body," said Seibert.
"CTA for evaluation of the renal arteries, evaluation of the aorta, the peripheral vascular system from the iliac down to the lower extremities, particularly down near the foot, is immediate, painless, and minimally invasive," agreed Truwit. "It is useful for diagnostic work to determine which patients actually need a dedicated angiogram with a catheter and a therapeutic procedure."
"CTA is incredible, especially with the new scanners that can get thinner and thinner sections, providing exquisite detail," added Rumberger. "It's replacing diagnostic catheterization and I believe that, in the future, it will replace diagnostic peripheral angiography."
Benefits of 3D technology
"The major benefit of 3D imaging is that it allows you to maximize the information transfer from the high-resolution volumetric CT data sets to the radiologist, and, most importantly, to the clinician," said Rubin. "It allows for characterization of disease that simply cannot be done by evaluating standard cross-sectional images."
"It allows a better appreciation of anatomic relationships," agreed Hartman. "It probably increases your sensitivity to pick up subtle abnormalities as well, at least to some degree. Typically, we make a diagnosis off the axial images, but sometimes there may be a subtle abnormality, such as a small aneurysm, that isn't obvious on the axial source images. When they are stacked together in the reconstruction, it becomes much more apparent."
"The ability to interact with the 3D volume data means that we can fine-tune the image on the fly and be directed to very accurately extract the information we need," said Newton. "In other words, it's possible just to dive into the volume, zoom up, and bring out the diagnostic information that you are seeking."
Potential pitfalls
"As with most things, there has to be a degree of caution in that this is not the be-all and end-all," said Hartman. "It still requires careful evaluation of the images to make sure that one isn't being fooled by the reconstruction. The reality is that 3D reconstruction is one more step away from what is really there, and every step away has the potential for misinformation or lost information. It definitely has some advantages, but ideally each application should be validated to ensure that there is some benefit. If something makes really pretty pictures but doesn't change the patient management, increase the accuracy of diagnosis, or allow the surgeons or other interventionalists to do things more rapidly or more safely, then, really, you are just making pretty pictures at the expense of radiation dose and contrast. As the largest nonnatural source of radiation to the general population, it is our responsibility as radiologists to keep that exposure as low as possible."
"In addition, 3D imaging is computationally intensive," added Newton. "We acquire so much information that must be managed. This requires
the horsepower of complex graphic workstations. Frankly, it provides us with more information than we know what to do with." "More information sometimes is better and sometimes is worse," agreed Nguyen, "especially if the information is inconclusive on the 3D image."
In addition, certain 3D procedures require a large bolus of contrast media, which can be a concern in patients who have underlying renal disease or in those with contrast sensitivity. There is also concern regarding increasing radiation dose with more frequent use of MDCT imaging. "There is a higher dose of radiation since we are using much thinner sections in some of these studies, especially for the aorta and lower-extrem-ity disease," said Hartman. "Generally, we believe that the end benefit outweighs the small theoretical risk from radiation, but it is something that should be used judiciously."
The future of 3D imaging
"What's happening today is that we, the radiology community, are being inundated with an unbelievable amount of information that must be synthesized within a finite amount of time," said Seibert. "Where I see 3D going in the future is being able to take that information content, make it more palatable and more concise, and being able to render this information with respect to using computer-aided detection and computer-aided display devices to allow the radiologist to interact with the dataset more effectively. In the future, I think we will see more and more emphasis on 3D rendering, not only with CT and MRI, but also with ultrasound, nuclear medicine, and the fusion of positron emission tomography (PET) and CT."
"I believe 3D imaging technology will continue to improve," said Hartman. "The scanners are already improving. I think that the diagnostic accuracy is already very high, but it still has a little bit of room for improvement. I think what's going to happen next is a greater dissemination of this technology. The 8-, 16-, or 64-slice systems are currently available at some institutions, but they are still relatively a minority. That technology will, I think, improve and will become increasingly available to smaller hospitals and, in turn, will become more widely available to the general patient population."
"What I see in the future is the ability to integrate 3D imaging with the intervention," said Poon, "so that when you scan the patient, you can get a 3D set of data and intervene immediately because you have a very precise image of where the pathology is located." "In the future, the shift will probably be more toward relying on the 3D image for the bulk of diagnosis and then reviewing the source images for problem solving or confirmation," said Hartman.
"It's mind boggling as to what can be done now with conventional, albeit very powerful, standard CTs," concluded Seibert. "Because of improvements in the user interfaces, the radiologists are taking these capabilities and using them on a day-to-day basis to make differential diagnoses and, more importantly, to describe and help the referring physicians to get the information that they need."
Will 3D imaging replace interventional radiology?
As the quality and detail of 3-dimensional (3D) computed tomographic (CT) images continues to improve and new imaging procedures are developed, the question becomes, "Will 3D imaging replace interventional radiology?"
According to the experts, the answer is yes…and no.
"Imaging studies have unquestionably replaced invasive diagnostic procedures," explained Geoffrey D. Rubin, MD, Chief of Cardiovascular Imaging and Associate Professor, Stanford University School of Medicine, Stanford, CA. "We used to perform a tremendous amount of diagnostic angiography but now we have almost completely replaced it with CT angiography (CTA)."
"It's something that's really changing the face of imaging, especially for vascular imaging," agreed Jonathan Hartman, MD, Assistant Professor of Radiology, Director of Neurointerventional Radiology, University of California, Davis, Sacramento, CA. "The standard for evaluation of the blood vessels is angiography, but there is risk associated with it. When I am doing a cerebral angiogram, I tell my patients there is no way of avoiding the fact that there is a risk of bleeding, infection, or stroke. All of these things usually don't happen, but there is no way to guarantee that won't happen. Whereas when we do a CTA and the 3D reconstruction, there is a small risk from the radiation, but overall it is a much safer study."
But for therapeutic interventional procedures, the story is different. "For interventional procedures where one is actually intervening, meaning putting in stents or performing angioplasty, that still has to be done interventionally," said Rubin, "3D imaging can definitely facilitate the guidance of these procedures but it can't replace the intervention." "You can't yet guide a catheter somewhere or put in coils with a CT scan," added Hartman, "but I would definitely say that 3D imaging is replacing a lot of the conventional angiography, as it should."
"I don't think at this time imaging will replace intervention," noted Daniel Nguyen, MD, Director of Neuroradiology and Director of 3D Imaging and Surgical Planning Services, Georgetown University Hospital, Washington, DC. "It will complement it. I would think that maybe someday if the technical challenges of CT scanners, basically the temporal and spatial resolution, can be overcome, then we can discuss it. But I don't think that we are there yet."
Vendors of 3D CT products
3D Software and Workstation Vendors
Able Software Corp
3D Doctor
5 Appletree Lane Lexington, MA 02420-2406
(781) 862-2804 www.ablesw.com
AccuImage Diagnostic Corp.
AccuView 3D Workstation
9400 Grandview Drive, Suite 201
South San Francisco, CA 94080
(650) 875-0192
www.accuimage.com
Barco
VesselMetrix, Voxar Colonscreen, Voxar 3D
3059 Premier Parkway
Duluth, GA 30097
(678) 475-8000
www.barco.com
Cedara Software Corp.
Cedara CT Works software
6509 Airport Road
Mississauga, Ontario L4V 1S7 Canada
(800) 724-5970 Fax: (905) 672-2307
www.cedara.com sales@cedara.com
Computmedics Neuroscan
Curry Neuroimaging Software
7850 Paseo Del Norte
El Paso, TX 79912
(877) 717-3975 (915) 845-5600
www.compumedics.com
E-Z-EM, Inc.
InnerviewGI Workstation
1111 Marcus Ave., Suite LL-26
Lake Success, NY 11042
(516) 333-8230 (800) 544-4624
Fax: (516) 302-2919
www.ezem.com
GE Healthcare
Advantage Workstation
3000 North Grandview Blvd.
Waukesha, WI 53188
(800) 886-0815
www.gehealthcare.com
Hermes Medical Solutions Inc.
Hermes Software
2865 South Charles Blvd.
Greenville, NC 27858
(866) HERMES 2
(252) 353-0050
Fax: (252) 353-0687
www.hermesmedical.com
info@hermesmedical.com
INFINITT Co, Ltd.
Rapidia 3D Workstation
TaeSuk Bldg, 9-10F 275-5,
Yangjae-Dong Seocho-Gu
Seoul, Korea 137-943
82-2-2194-1600 Fax: 82-2-2194-1699
www.infinitt.com
Mercury Computer Systems
Amira
12626 High Bluff Drive, Suite 200
San Diego, CA 92130
(858) 794-1600 (858) 523 1094
3d_info@mc.com
MillenTech Systems
Vision Tools 3D CTview software and workstation
12 Obour Buildings
Salah Salem St.
Cairo, Egypt 11731
201-2-342-1185 Fax: 202-260-6414
sales@millentech-systems.com
Philips Medical Systems
EasyVision Endo software
22100 Bothell Everett Highway
P.O. Box 3003-98041-3003
Bothell, WA 98021-8431
(800) 229-6417
www.medical.philips.com
ScImage
NetraMD 3D workstation and PICOMEnterprise software
4916 El Camino Real
Los Altos, CA 94022
(866) SCIMAGE
(650) 694-4858
www.scimage.com
corporate_sales@scimage.com
Siemens Medical Solutions USA, Inc.
syngo 3D software
51 Valley Stream Parkway
Malvern, PA 19355
(888) 826-9702
www.usa.siemens.com/medical
e.health@sms.siemens.com
TeraRecon, Inc.
Aquarius workstation
2955 Campus Dr., Suite 300
San Mateo, CA 94403
(650) 372-1100 Fax: (650) 372-1101
www.terarecon.com
info@terarecon.com
Viatronix, Inc.
V3D System workstation
25 Health Sciences Dr., Suite 203
Stonybrook, NY 11790-3350
(631) 444-9700
www.viatronix.com
medical@viatronix.com
Vital Images, Inc.
Vitrea 2 3D Workstation
5850 Opus Parkway, Suite 300
Minnetonka, MN 55343
(952) 487-9500
(800) 231-0607 Fax: (763) 852-4110
www.vitalimages.com
3D CT Scanner Vendors
GE Healthcare
GE LightSpeed with Direct 3D
3000 North Grandview Blvd.
Waukesha, WI 53188
(800) 886-0815
www.gehealthcare.com
Philips Medical Systems
Brilliance Workspace
22100 Bothell Everett Highway
P.O. Box 3003-98041-3003
Bothell, WA 98021-8431
(800) 229-6417
www.medical.philips.com
Shimadzu Medical Systems
SCT-7800 Series
20101 South Vermont Ave.
Torrance, California 90502
(310) 217-8855, (310) 217-0661
www.Shimadzumed.com
information@shimadzumed.com
Siemens Medical Solutions USA, Inc.
SOMATOM
51 Valley Stream Parkway
Malvern, PA 19355
(888) 826-9702
www.usa.siemens.com/medical
e.health@sms.siemens.com
Toshiba America Medical Systems
Aquillion CT scanner
2441 Michelle Drive
Tustin, CA 92780
(800) 421-1968
www.medical.toshiba.com
mkttcomm@tams.com
Notes
- This list includes only products that currently have FDA approval for marketing in the United States. Other products are currently in development and may be available for purchase in the United States in the future.
- A number of universities and academic medical centers have developed or are in the process of developing their own 3D CT software or image utilities. Some of these products may be available for research purposes or for purchase for clinical use in the United States now or in the future.
- This vendor information is as accurate and complete as possible at press time. Whenever possible, details were confirmed with the vendors.
- Any omission of a product or vendor is unintentional.
Related Articles
Citation
Applied Radiology Focus: Three-dimensional image rendering for CT. Appl Radiol.
March 10, 2005