Talocalcaneal Coalition
Images


Case Summary
A teen track runner presented with a 5-month history of left foot and anterior ankle pain. On physical examination, there was tenderness in the anterolateral ankle, negative anterior drawer test to assess the lateral collateral ligaments, negative varus tilt test to evaluate for a sprain of the anterior talofibular ligament, and a flat-appearing foot with a positive heel raise suggesting posterior tibial tendon dysfunction. Range of motion of the ankle was normal. The Foot and Ankle Measure Activities of Daily Living Score (ADL) (to assess physical function) and Sports Score (SS, a performance measure) were 83.33% and 87.5%, respectively. The ADL score is on the cusp between fair and good function, while the SS indicates that ankle performance is abnormal (greater than 10% below the patient’s normal ankle).
Imaging Findings
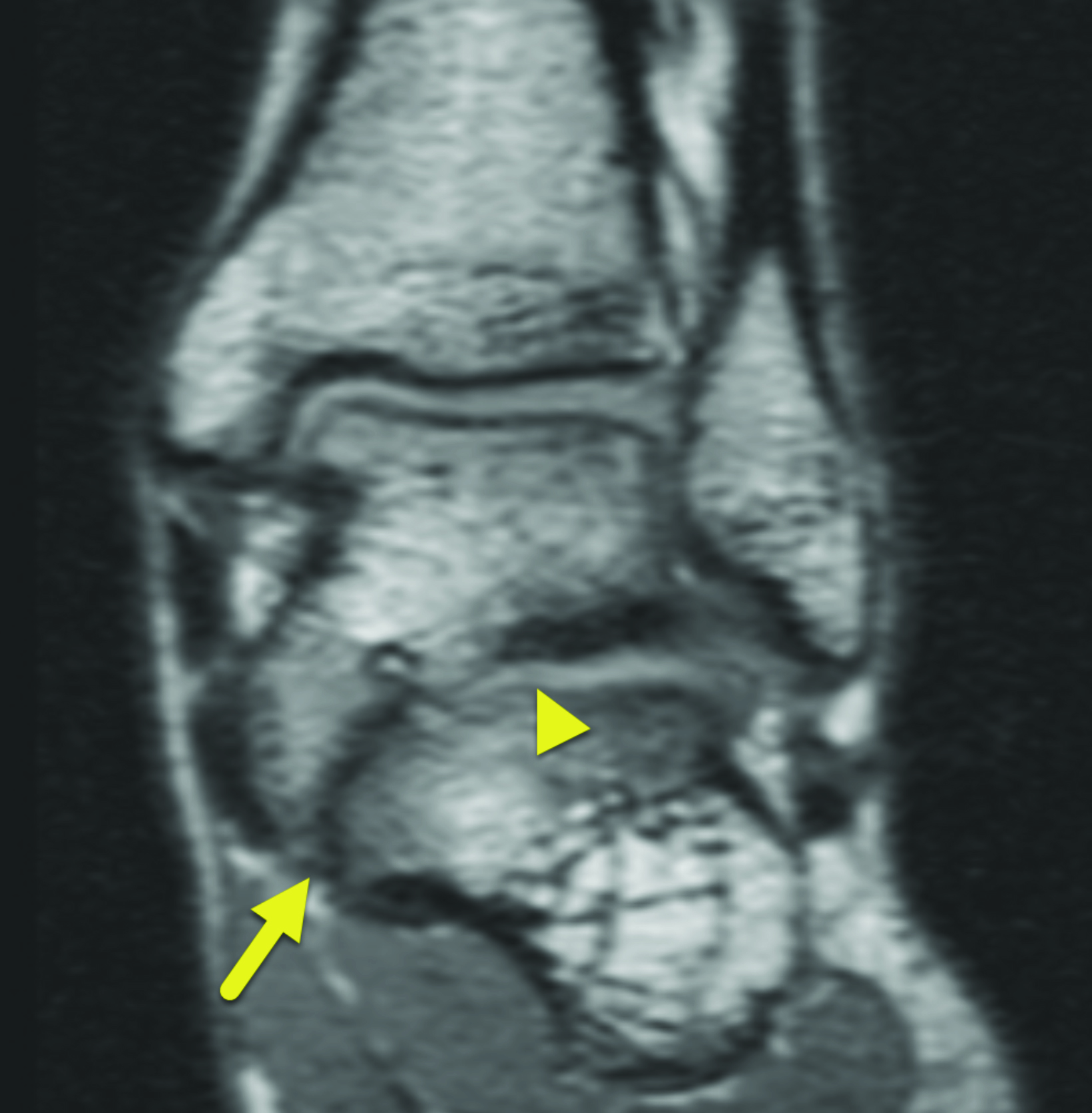
Left ankle radiographs showed talocalcaneal coalition (Figure 1). Magnetic resonance imaging (MRI) of the left foot (Figure 2) revealed a mixed osseous and fibrocartilaginous talocalcaneal coalition across the medial talocalcaneal facet with associated joint narrowing, abnormal downward sloping of the medial facet of the subtalar joint, subchondral bony irregularity, and subcortical bone marrow edema across the facet. There was also associated talar beaking and hypoplasia of the sustentaculum tali and a stress reaction of the base of the 2nd and 3rd metatarsal.
Diagnosis
Talocalcaneal coalition (involving the medial talocalcaneal facet).
The differential diagnosis for an anterior or posterior ankle pain includes sprains, calcaneonavicular coalition, pes plenovalgus, and a subtalar joint tumor.1 Radiography, MRI, computed tomography (CT) and ultrasound can all aid in identifying talocalcaneal coalition.2-5
Discussion
Tarsal coalition is a general term that refers to fusion of the bones of the foot. It is a common cause of painful flat foot and foot pain in adolescents and can be osseous, cartilaginous, fibrous, or a mixture of these elements.6 It most commonly affects the calcaneonavicular joint or the talocalcaneal joint. Tarsal coalition is present in 1-2% of the population.1 It can occur in isolation or as part of a genetic syndrome. Talocalcaneal coalition most commonly affects the middle facet of the subtalar joint.1
About 75% of patients with talocalcaneal coalition are asymptomatic. Symptomatic patients generally present between 12 and 15 years of age with pain on the anterior and dorsal aspects of the ankle that is exacerbated by movement and weight bearing. There can also be calf pain resulting from reactive tightening of the gastrocnemius and soleus muscles. Talocalcaneal coalitions cause depression of the medial longitudinal arch and lead to the appearance of a flat foot on physical exam.1 Lastly, a prominence on the medial malleolus can be palpated which represents an enlarged medial facet and is referred to as the double medial malleolus sign.4
On radiography and CT, findings of talocalcaneal coalition include the continuous C-sign, talar break, humpback sign, and duck-face sign. The continuous C-sign is present in all types of talocalcaneal coalition. It is visible on the lateral view and is seen as a C-shaped arc extending from the talar dome along the posterior/inferior edge of the sustentaculum tali. Normally, the subtalar joint disrupts this arc. However, with coalition, the C-shaped arc is continuous. The talar beak sign is an osseous protuberance on the anterior and distal talar neck; the humpback sign represents a protuberance arising from the posterior aspect of the subtalar joint. Finally, the duck-face sign is seen as a protuberance of the medial talocalcaneal joint on the AP view.5
On physical exam, the bony protuberance seen as part of the duck face sign can give the appearance of a double medial malleolus. This appearance can also be seen on CT When present, the double medial malleolus is 81% sensitive and 79% specific for a diagnosis of talocalcaneal coalition.4
On MRI, findings include the presence of bone marrow edema in the articulation area, facet joint hypertrophy, narrowing of the joint space, and irregularities within the articular surfaces or joint spaces.3 In osseous coalitions bone marrow signal will continue across the coalition.
Typically, there is high T1 and low T2 signal in the fused area. However, the cartilaginous and fibrous coalitions have a narrowed joint space at the site of the coalition, irregularity of the bone interface and often bone marrow edema. Cartilaginous coalitions will have signal intensity like fluid or cartilage with intermediate T1 signal and intermediate to high signal. while fibrous coalitions will demonstrate low signal intensity on all sequences across the abnormal joint.7
First-line treatment for talocalcaneal coalition includes rest and periods of immobilization, which generally relieve the symptoms. However, when these measures do not provide relief, surgical resection can be performed. Though surgical coalition resection was previously considered controversial, recent studies have demonstrated otherwise.8,9 Di Gennaro, et al, showed that patients who underwent resection had a significantly increased American Orthopaedic Foot and Ankle Society – Ankle Hindfoot Score and Foot and Ankle Disability Index as compared to patients who did not undergo surgery.
Conclusion
Talocalcaneal coalition is an isolated or syndromic condition that is typically asymptomatic. Symptomatic patients generally present with repeated ankle sprains, ankle pain, and a flattened foot. Generally, first-line treatment includes rest and immobilization, with surgical consideration given to refractory cases. Recent studies highlight the efficacy of surgical coalition resection over traditional treatment with a better patient outcome and a low rate of complications.
References
- Guduri V, Dreyer MA, Talocalcaneal Coalition. in StatPearls. 2020: Treasure Island (FL).
- Bianchi S, and Hoffman D, Ultrasound of talocalcaneal coalition: retrospective study of 11 patients. Skeletal Radiol. 2013. 42(9): 1209-1214.
- Umul A. MRI Findings of talocalcaneal coalition: two case reports. Acta Inform Med. 2015; 23(4): 248-249.
- Rocchi V, et al. The “Double Medial Malleolus”: a new physical finding in talocalcaneal coalition. J Pediatr Orthop. 2018; 38(4): 239-243.
- Lee, SH, et al. Talocalcaneal coalition: A focus on radiographic findings and sites of bridging. Indian J Orthop. 2016; 50(6): 661-668.
- Berzins U, et al. Talocalcaneal coalition including open comminuted calcaneal fracture: a case report and literature review. Bull Emerg Trauma. 2019; 7(1): 80-83.
- Lawrence DA, Rolen MF, Haims AH, Zayour Z, Moukaddam HA. Tarsal coalitions: radiographic, CT, and MR imaging findings. HSS J. 2014;10(2):1533-1566. doi: 10.1007/s11420-013-9379-z. Epub 2014 Feb 12. PMID: 25050099; PMCID: PMC4071469
- Di Gennaro GL, et al. Operative versus nonoperative treatment in children with painful rigid flatfoot and talocalcaneal coalition. BMC Musculoskelet Disord. 2020; 21(1): 185.
- Aibinder, W.R., E.Y. Young, and T.A. Milbrandt. Intraoperative three-dimensional navigation for talocalcaneal coalition resection. J Foot Ankle Surg. 2017; 56(5):1091-1094.
Citation
N V, RB T, CM S, Y L, AJ T.Talocalcaneal Coalition. Supplement to Applied Radiology. 2022; (6):15-17.
November 2, 2022