Rib Osteochondromas Mimicking Lung Nodules
Images
CASE SUMMARY
A 12-year-old with known hereditary exostoses presented with a one-month history of intermittent right-sided chest pain.
IMAGING FINDINGS
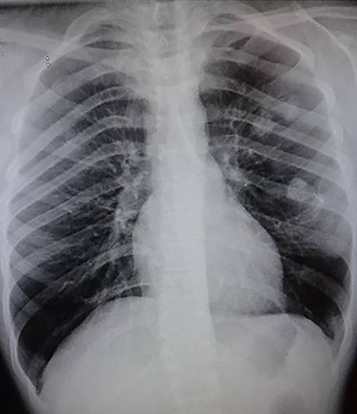
A chest radiograph (Figure 1) revealed two nodules projecting over the left upper lung field and one larger nodule projecting over the left middle lung field. A thin linear density could be appreciated, extending laterally from the larger nodule. The lungs were otherwise clear. The pleural spaces were clear. The mediastinal contour and cardiac silhouette appeared within normal limits. There was a small suspected exostosis off of the right posterior third rib and an exostosis noted off of the right scapula.
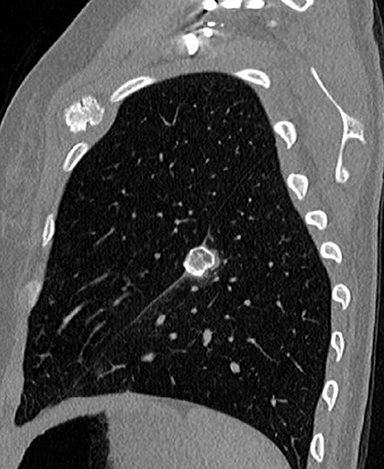
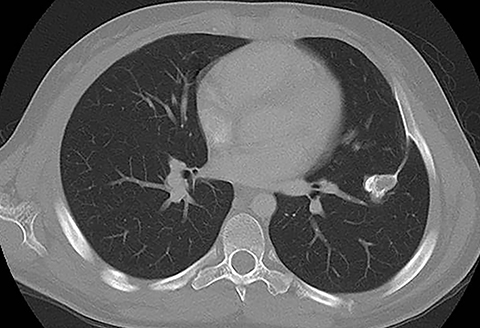
A subsequent contrast-enhanced CT performed to further assess the suspected pulmonary nodules revealed multiple bony exostoses arising from all the ribs, the vertebrae included in the scan, and the clavicles, as well as the scapula, sternum, and proximal humeri. A calcified structure measuring approximately 2.4 × 1.8 × 1.6 cm was centered in the left pulmonary fissure with a long, thin stalk extending laterally within this fissure to the lateral aspect of the left fifth rib (Figure 2). This lesion corresponded to the largest apparent “lung nodule” on chest X-ray. An additional calcified structure with a lobulated appearance measuring approximately 3.0 × 1.8 × 2.0 cm was seen arising from the anterior aspect of the left second rib (Figure 2). This lobulated structure likely accounted for the additional nodules projecting over the left upper lung on the chest X-ray. Given that the patient’s chest pain was on the contralateral side, the large osteochondromas described here were likely asymptomatic at this stage.
DIAGNOSIS
Rib osteochondromas mimicking lung nodules
DISCUSSION
Osteochondromas, or exostoses, are benign, cartilage-capped bone tumors with continuous cortex and marrow extending from the underlying bone. Osteochondromas may be solitary or multiple. When multiple, these lesions are associated with the autosomal dominant syndrome, hereditary multiple exostoses (HME).1 Patients with HME typically present with osteochondromas of the costal bones (40%), proximal humerus (50%), distal femur (70%), and proximal tibia (70%).2 Complications associated with osteochondromas are more frequent with HME; they include deformity (cosmetic and osseous), fracture, vascular compromise, neurologic sequelae, overlying bursa formation, and malignant transformation.1
Several case reports have described costal osteochondromas as a cause for thoracic injury, including hemothorax and pneumothorax.3-6 Chronic pleural effusion7,8 and pleuritic chest pain9 secondary to chondral osteochondromas have also been reported.
CONCLUSION
We present a case of hereditary exostoses with a large pedunculated osteochondroma within the left pulmonary fissure mimicking a pulmonary nodule. In the setting of apparent pulmonary nodules and known HME, identifying a bony stalk extending from the “pulmonary nodule” to an adjacent bone may obviate the need for further assessment with chest CT.
REFERENCES
- Murphet MD, Choi JJ, Kransdorf MJ, Fleming DF, Gannon FH. Imaging of Osteochondroma: Variants and Complications with Radiologic Pathologic Correlation. RadioGraphics. 2000; 20:1407–1434.>
- Schmale GA, Conrad EU, Raskind WH (1994) The natural history of hereditary multiple exostoses. J Bone Jt Surg Am. 76(7):986–992.
- Mann E, Kaafarani HM, Cassidy C, Chwals WJ, Jackson CC. Spontaneous hemothorax in multiple exostoses: a case report and review of literature. J Laparoendosc Adv Surg Tech.2011; 21:575–577.
- Khosla A, Parry RL. Costal osteochondroma causing pneumothorax in an adolescent: a case report and review of the literature. J Pediatr Surg. 2010; 45:2250–2253.
- Pham-Duc ML, Reix P, Mure PY et al. Hemothorax: an unusual complication of costal exostosis. J Pediatr Surg. 2005;40:e55–e57.
- Harrison NK, Wilkinson J, O’dononohue et al. Osteochondroma of the rib: an unusual cause of hemothorax. Thorax. 1994;46:618-619.
- Chen J, Nelson S, Tzung B, Applebaum H, De Ugarte DA. Costal osteochondroma spicule associated with pleural effusion. Pediatr Surg Int. 2014; 30:357–359.
- Yan G, Littlewood A, Latimer MD. Unusual cause of pleuritic chest pain in a child. BMJ Case Reports. 2016; doi:10.1136/bcr-2016-217307
- Ghoneim A, Kejriwal N. Unusual Cause of Persistent Chest Pain. Heart, Lung Circ. 2016;25:e168–e169.
Citation
G S, C R.Rib Osteochondromas Mimicking Lung Nodules. Appl Radiol. 2021; (1):56A-56B.
January 19, 2021