Retrograde Jejunogastric Intussusception and Novel Reduction
Images



CASE SUMMARY
A middle-aged adult presented to the emergency department with acute onset of colicky epigastric pain, nausea and vomiting. The symptoms had started shortly after eating lunch. The patient had undergone a Whipple procedure three years earlier for resection of a pancreatic neuroendocrine tumor. Physical examination revealed a palpable, tender fullness in the left upper abdomen.
IMAGING FINDINGS
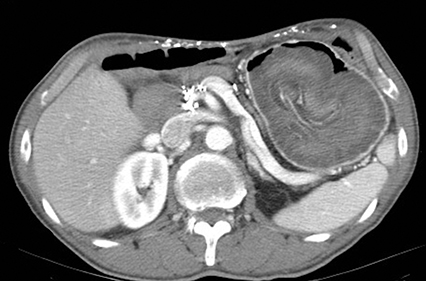
A supine radiograph of the abdomen showed pneumobilia and surgical staples related to the prior surgery. A contrast-enhanced CT of the abdomen demonstrated an 8 x 10 cm lobulated, soft-tissue mass within the stomach (Figure).
The appearance of the mass and superior mesenteric vessel blood supply indicated that a loop of proximal jejunum had protruded through the wide gastrojejunal anastomosis and become entrapped inside the gastric pouch.
Based on the well-established success of air enema to reduce colonic intussusception, the patient was asked to ingest 12 ounces of an effervescent soft drink to produce gas and elevate the stomach’s intraluminal pressure.
Within 10 minutes the patient experienced a sudden gastric cramp followed by complete symptom relief. Subsequent endoscopy showed a widely patent gastrojejunostomy and slightly hyperemic mucosa of the efferent loop.
DIAGNOSIS
Retrograde jejunogastric intussusception
DISCUSSION
Jejunal intussusception is an uncommon but well-documented complication of gastrojejunostomy performed during Billroth II operation or Roux-en-Y gastric bypass for morbid obesity.1-3 It occurs as jejunojejunal intussusception in the majority of cases.4
Simper, et al, reviewed their experience with over 15,000 patients who had undergone Roux-en-Y gastric bypass surgery.2 They found that 22 had developed jejunojejunal intussusception, but only one had retrograde jejunogastric intussusception. However, other authors have mentioned that almost 200 examples of retrograde jejunogastric intussusception are recorded in the medical literature, either as isolated cases or as small series.3-6 The latter complication appears to be very rare after a Whipple procedure, although one such case has been reported recently.7
Postsurgical retrograde jejunogastric intussusceptions may involve the afferent loop (Type I), efferent loop (Type II), or a combination of both (Type III).1,8 Type II accounts for 80% of cases, as in our case, whereas the other types account for 10% each. It has been postulated that reversed antiperistaltic contractions of the anastomosed jejunal segment caused by vomiting, or some other mechanical factors such as adhesions and surgical sutures or staples, may induce retrograde intussusception into the gastric pouch.1,3,8
Acute jejunogastric intussusception can develop within a few weeks after surgery or several years later as in this case.1,5 There is also a chronic recurrent type that tends to resolve spontaneously. It should also be noted that the abdominal symptoms caused by such intussusceptions are often similar to that of iatrogenic internal hernias, which may occur after various types of gastrojejunal anastomosis.3,9
As reported in several publications, radiological diagnosis of this complication can be made by upper GI examination, sonography, or abdominal CT.1-3,6-8 Although some may reduce spontaneously, most patients require prompt endoscopic or surgical intervention, since delayed treatment can lead to ischemic infarct of the invaginated loop.1,3,7 In this case, however, gastric distention with gas via an effervescent soft drink proved a simple and effective therapy.
This technical approach is somewhat similar to the successful application of air enema for pneumatic reduction of colonic intussusception.10 It may also be useful for conservative management of an uncomplicated gastrojejunal intussusception if recognized early.
CONCLUSION
Retrograde jejunogastric intussusception is a rare complication of Whipple procedures, but it occurs more frequently after Billroth II gastrojejunostomy or Roux-en-Y gastric bypass for morbid obesity. The presenting symptoms are acute epigastric pain, nausea, vomiting, hematemesis, and a palpable, tender mass in the hypochondrium.
Radiology plays a crucial role in differentiating this entity from a postoperative internal hernia and enabling prompt treatment to prevent catastrophic infarction of the intussuscepted intestinal loop.
REFERENCES
- Hammond N, Miller FH, Dynes M. Intussusception into the enteroanastomosis after Billroth II gastrectomy and Roux-en-Y jejunostomy: sonographic and CT findings. Am J Roentgenol. 2001; 177:624-626.
- Simper SC, Erzinger JM, McKinlay RD, et al. Retrograde (reverse) jejunal intussusception might not be such a rare problem: a single groups’s experience of 23 cases. Surg Obes Relat Dis. 2008; 4(2):77-83.
- Pande R, Fraser J, Harmston C. Emergency presentation of retrograde intussusception as a late complication of gastric bypass. Ann R Coll Surg Engl. 2012; 94(3): 116-
- Daellenbach L, Sutter M. Jejunojejunal intussusception after Roux-en-Y gastric bypass: a review. Obes Surg. 2011; 21:253-263.
- Genser L, Pattou F, Caiazzo R. Retrograde jejuno-jejunal intussusception 7 years after a Roux-en-Y gastric bypass. J Visc Surg. 2015; 152(2): 137-139.
- Kawano F, Tashiro K, Nakao H, et al. Jejunogastric intussusception after distal gastrectomy with Roux-en-Y reconstruction: a case report. Int J Surg Case Rep. 2018; 44:105-109.
- Patel K, Luthra A, Aberra F, et al. Intussusception after pancreaticoduodenectomy. ACG Case Rep J. 2019; 6(5):60-62.
- Singh S, Singh A, Bhagat S, et al. Retrograde jejuno-gastric intussusception. Niger J Surg. 2015; 21(1): 70-72.
- Higa KD, Ho T, Boone KB. Internal hernias after laparoscopic Roux-en-Y gastric bypass: Incidence, treatment and prevention. Obes Surg. 2003; 13(3):350-354.
- McDermott VG, Taylor T, Mackenzie S, et al. Pneumatic reduction of intussusception: clinical experience and factors affecting outcome. Clinical Radiology 1994; 49 (1):30-34.
References
Citation
GG G.Retrograde Jejunogastric Intussusception and Novel Reduction. Appl Radiol. 2021; (5):53-54.
September 10, 2021