Radiological Case: Intra-abdominal pregnancy
Images





CASE SUMMARY
A 24-year-old, primigravida woman was referred at 28 weeks gestational age for Doppler studies to rule out intrauterine growth retardation. She had undergone regular obstetric follow up elsewhere, including a dating scan which confirmed a single live intrauterine gestation with adequate interval growth. At 2 months amenorrhea she gave a history of acute abdominal pain associated with spotting per vaginum. Emergency ultrasound done elsewhere at that time confirmed the presence of single live intrauterine gestation. She was given hormonal support and advised to remain on bed rest. Her pregnancy continued uneventfully until she went to a nearby government hospital for a routine checkup, when she was clinically diagnosed as IUGR and referred to our institute for fetal Doppler evaluation.
IMAGING FINDINGS
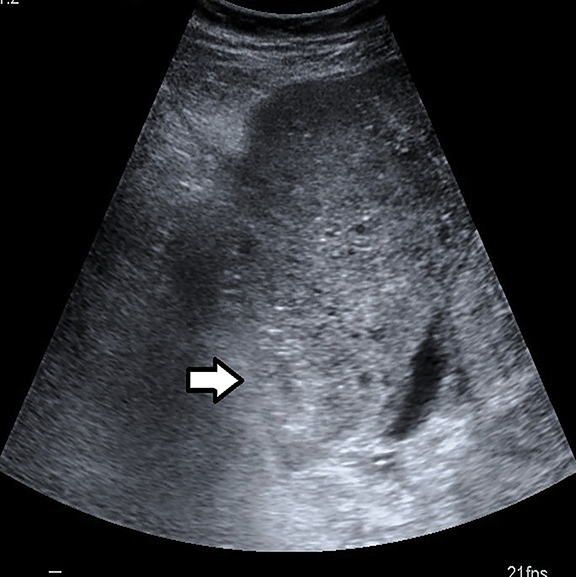
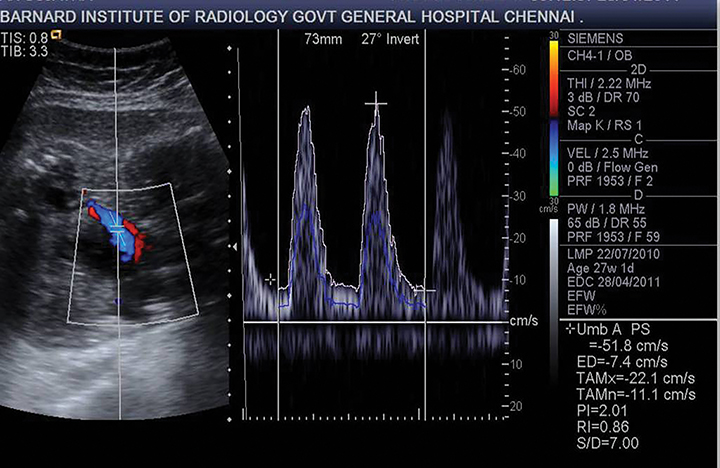
Real-time sonography demonstrated a single live fetus in transverse lie with the fetal head in left lumbar region.The bulky empty uterus was seen separately in the pelvis posterior to the bladder (Figures 1,2). There was no demonstrable uterine myometrium around the fetus (Figure 3). Fetal biometric data was consistent with 23-24 weeks gestation as opposed to the expected gestational age of 27-28 weeks. Amniotic fluid was scanty (Figure 4). The placenta was localized to the right hypochondrium (Figure 5), with minimal free fluid in the Pouch of Douglas. As a separate uterus was identified away from the fetus, the possibilities of pregnancy in a uterine diadelphys or pregnancy in a uterine horn were considered. But the absence of myometrial tissue around the fetus and presence of free fluid in POD outlining the fetal head without intervening myometrium (Figure 3) ruled out these possibilities. Consequently, a diagnosis of intra-abdominal pregnancy was made. Doppler US of the umbilical artery revealed a high resistive index of 8 (Figure 6).
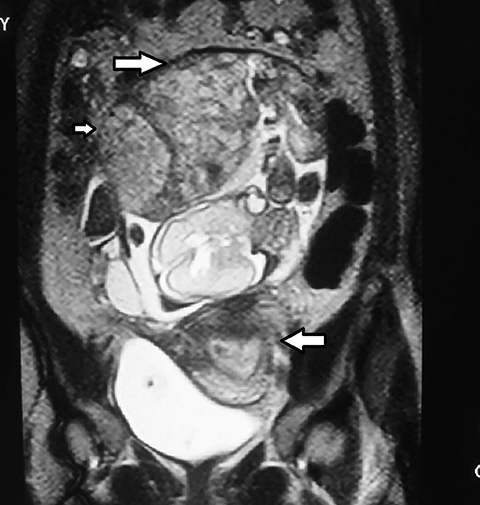
An MRI examination was subsequently performed with a 1.5T Siemens Emotion Duo in all three orthogonal planes with HASTE sequence. A fetus surrounded by a thin amniotic membrane was demonstrated to lie in the transverse position within the abdominal cavity (Figure 7). No myometrium was visualized around the fetus. The placenta was seen in the right hypochondrium with displacement of adjacent maternal bowel loops and implantation into fat intensity structure possibly omentum (Figure 8). Very few amniotic pockets were seen surrounding the fetus. The maternal urinary bladder, rectum and bowel loops were found to be relatively free of the fetal sac. The uterus was found separately in the pelvis with its posterosuperior wall adhering to the fetal sac.
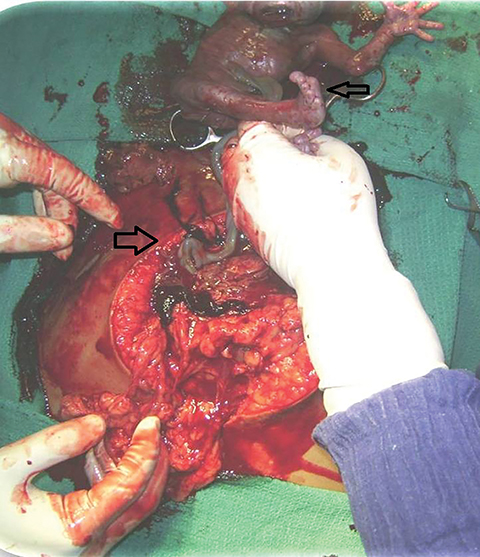
In view of severe fetal IUGR and high risks associated with continuing the pregnancy, the patient was advised to terminate her pregnancy. Accordingly, a laparotomy was performed. Preoperative findings matched our antenatal imaging findings (Figure 9). A live IUGR male baby weighing approximately 500 g with Apgar 4/10, 6/10 was delivered and shifted to the NICU for ventilator support. The placenta, still attached to the omentum, was released with difficulty. There were dense adhesions between the posterosuperior aspect of the uterus and the amniotic membrane. The right tube and ovary were found to be normal while the left tube and ovary could not be visualized because of dense adhesions. The placenta was removed in toto and the abdomen closed in layers. Four units of blood were transfused intraoperatively. The postoperative period was uneventful.
DIAGNOSIS
Intra-abdominal pregnancy
DISCUSSION
Intra-abdominal pregnancy is a type of ectopic pregnancy wherein the fetus grows in the abdominal cavity. The extrauterine implantation can occur in the omentum, the large vessels or even in the vital organs. Abdominal pregnancies account for 0.1% of all pregnancies and up to 1.4% of ectopic pregnancies.1 These pregnancies can go undetected until an advanced gestational age and often result in massive hemorrhage.2 Rates of maternal mortality range between 2 and 30%3. Advanced abdominal pregnancy carries a risk of hemorrhage, disseminated intravascular coagulation, bowel obstruction and fistulae to the gastrointestinal and/or genitourinary tracts.3 The site of implantation and availability of vascular supply determine the possibility of fetal survival. Risk factors associated with abdominal pregnancy include tubal damage, pelvic inflammatory disease, endometriosis, assisted reproductive techniques and multiparity. Clinical history and physical examination alone may be insufficient to make a preoperative diagnosis. Sonography is the most effective method for diagnosing an abdominal pregnancy. MRI is an emerging important, complementary imaging modality that helps not only to confirm the diagnosis but also to delineate the precise anatomical relationship between the fetus and various maternal abdominal organs.
Abdominal pregnancy occurs either as a result of tubal abortion or rupture (secondary abdominal pregnancy) or rarely as a result of primary peritoneal implantation (primary abdominal pregnancy). 1Primary peritoneal implantation is rare. Studdiford established three criteria for diagnosing primary peritoneal pregnancies: (1) normal bilateral fallopian tubes and ovaries; (2) the absence of uteroperitoneal fistula; and (3) a pregnancy related exclusively to the peritoneal surface and early enough to eliminate the possibility of secondary implantation following a primary nidation in the tube.4
The mortality of abdominal pregnancy is 7.7 times higher than that of tubal pregnancy and 90 times greater than that of intrauterine pregnancy.5 Associated morbidities include hemorrhage, disseminated intravascular coagulation, bowel obstruction and fistulae formation due to fetal bones protruding through thin amniotic membranes. Fetal malformations such as torticollis, facial asymmetry, malformation of limbs, flattening of the head and thorax, etc., may occur due to severe oligohydramnios.2
Abdominal pain is the most frequent symptom. Rarely, symptoms may relate to placental site attachment, including attachment to the bowel or bladder obstruction.
Sonographic features denoting abdominal pregnancy include fetus being seen outside the uterine cavity, absence of the uterine wall between bladder and fetal parts, oligohydramnios, fetal parts located close to the maternal abdominal wall, and abnormal location of placenta outside the uterine cavity.5 Sonography remains the imaging modality of choice for the evaluation of abdominal pregnancy when abnormal relationships among the fetus, uterus, placenta and amniotic fluid are made.6 It is also useful in assessing fetal congenital malformations usually associated with abdominal pregnancies.
The role of MRI is to locate the placenta and identify its adherence to any vital organs, including the liver and spleen. In this case, MRI not only helped confirm the diagnosis, but it delineated the exact anatomical localization of fetal parts and placental tissue as well as the adhesions to the uterus. This information proved vital in preoperative planning. The information on the location, state of viability of the placenta and blood supply will influence management and aid in planning surgery.7 MRI has many advantages over ultrasound as bone, gas-filled structures and maternal obesity provides no hindrance to imaging.
Preoperative angiograms can be useful in locating all sources of vascular supply to the placenta and if possible to embolize vessels difficult to ligate operatively. If the placenta is not removed during laparotomy, postoperative embolization of feeding arteries can be done to control hemorrhage from adherent placenta.5
Previous scans of our patient were read as an intrauterine pregnancy. She also had a history of first-trimester abdominal with spotting per vaginum, which might have been due to either a tubal abortion or a tubal rupture with the conceptus getting implanted into the peritoneal cavity.This had gone unnoticed with the fetus growing as an abdominal pregnancy. Approximately 50% of ectopic pregnancies are missed at the time of initial presentation. Advanced abdominal pregnancy is rare and accounts for 1 in 25,000 pregnancies.8
The management of abdominal pregnancy depends on fetal viability, presence of fetal congenital abnormalities, fetal gestational age, maternal complications, placental location and adherence. Usually surgical intervention is necessary regardless of fetal viability. The management of the placenta is still under debate. Total removal is preferable with ligation of blood supply or preoperative embolization. Partial removal due to adherence may result in massive hemorrhage and shock.3 In cases of adherence the placenta can be left in situ, ligating the cord as close to the placenta as possible. The placenta usually ceases to function after 4 months.2 Postoperative angiographic embolization of feeder vessels is possible and placental involution can be followed by serial bHCG. Some authors advocate preoperative systemic methotrexate in the management of abdominal pregnancy.9
REFERENCES
- Bertand G,Le R, Simard-Emond L, et al. Imaging in the management of abdominal pregnancy: A case report and review of the literature. JOGC.2009: 57-62.
- Kun KY, Wong PY, Ho MW, et al. Abdominal pregnancy presenting as missed abortion at 16 weeks’ gestation. HKMJ 2000;6:425-427.
- Parekh, VK, Bhatt S, Dogra VS. Adominal pregnancy: An unusual presentation. Journal Ultrasound Med. 27:679-681.0278-4297.
- Studdiford WE. Primary peritoneal pregnancy.Am J Obstet Gynecol.1942;44:487–491.
- Allibone, GW, Fagan CJ, Porter SC. The sonographic features of intra-abdominal pregnancy. Journal of Clinical Ultrasound. 1981 9(7): 383-387.
- Cohen JM, Weinreb JC, Lowe TW, et al. MR imaging of a viable full-term abdominal pregnancy.AJR.1985; 9:407-408.
- Tang HC, Kumar G, Ramli NM. A viable secondary intra abdominal pregnancy resulting from rupture of uterine scar. The Brit J Radiol.2007; 80: e 134 –e 136.
- Lastra A, Ruiz Bedoya JA, Jiménez Balderas EA. Abdominal pregnancy with fetal survival. A report of 2 cases.GinecolObstet Mex.1993; 61:348–350.[Pub Med]
- Gupta P, Sehgal A, Huria A, Mehra R. Secondary abdominal pregnancy and its associated diagnostic and operative dilemma: Three case reports. J Med Case Reports.2009;3:7382.Published online 2009 August 7.doi:10.4076/1752-1947-3-7382.
Citation
Radiological Case: Intra-abdominal pregnancy. Appl Radiol.
May 7, 2015