Primary Breast Lymphoma
Images


CASE SUMMARY
A middle-aged female who presented with a palpable mass in the left breast was found to have a small mass in left axilla on examination. There was no evidence of nipple discharge, retraction, skin erythema, or thickening. Patient had a history of hypertension, as well as a right breast mass with benign pathology in adolescence. Prior mammogram reported as BIRADS-2. The patient denied personal and family history of breast or ovarian cancer.
IMAGING FINDINGS
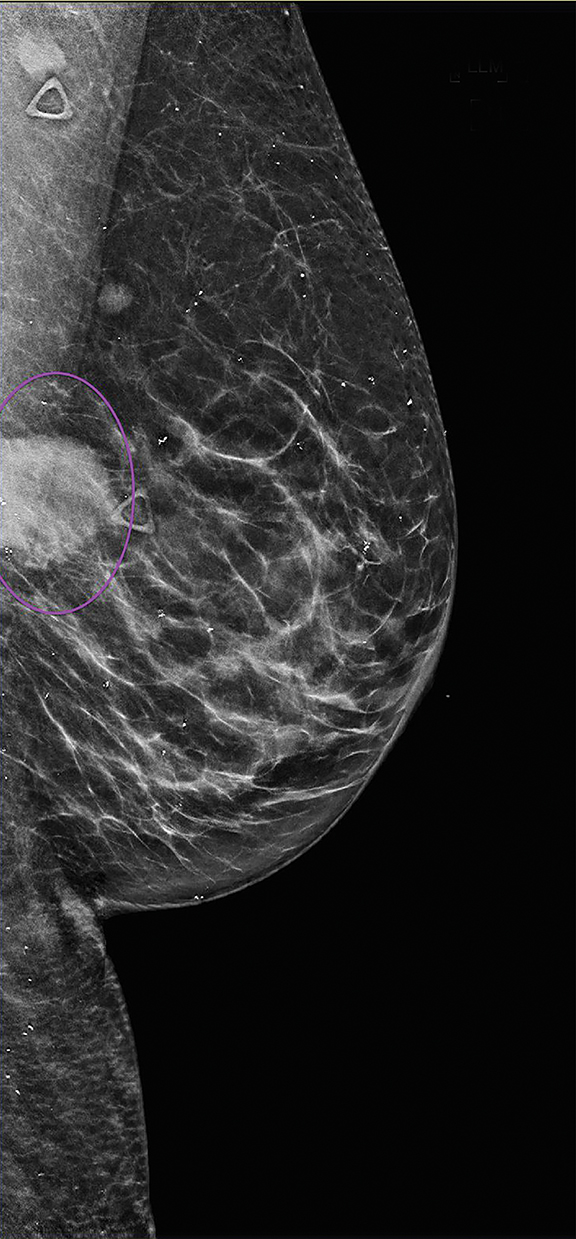
Mammography of the right breast revealed no suspicious grouping of micro-calcifications, developing masses, or areas of architectural distortion. Mammography of the left breast revealed interval development of a round, circumscribed, high-density mass in left central outer breast posterior depth at approximately the 3 o’clock position, corresponding to the palpable marker (Figure 1).
Diffuse calcifications were noted but no suspicious calcifications or architectural distortion. Additionally, an oval, high-density mass was seen in the left axilla, likely a lymph node, measuring 0.9 cm and corresponding to the other marker of a palpable mass (Figure 1). Findings were highly suspicious for malignancy; the patient underwent targeted ultrasound for the palpable abnormalities.
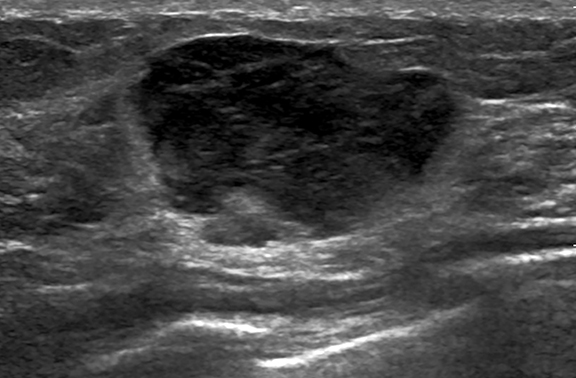
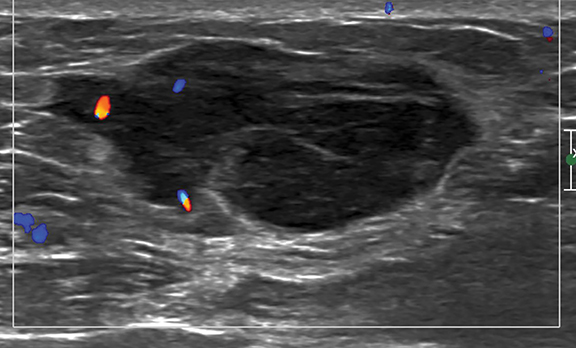
Targeted sonographic examination performed corresponding to the palpable breast abnormality revealed an oval, parallel, hypoechoic mass with predominantly microlobulated margins and medially angular margins (Figure 2). The mass measured 3.6 2.8 1.7 cm and was accompanied by mild internal and peripheral vascularity (Figure 2). A few axillary lymph nodes were seen, with the largest measuring 1.3 0.7 cm with cortical thickness measuring 0.5 cm, corresponding to the palpable mass in axilla.
The patient subsequently underwent ultrasound-guided core biopsy of the left breast mass and fine needle aspiration of the suspicious left axillary lymph node. Core biopsy from breast mass was consistent with follicular lymphoma Grade 3A. Axillary lymph node fine needle aspiration demonstrated normal lymphoid tissue.
DIAGNOSIS
Primary breast lymphoma. Differential diagnoses include invasive lobular carcinoma, metastasis to the breast, and phyllodes tumor.
DISCUSSION
Mammary lymphoma, a hematologic malignancy of the breast, is a rare entity with prevalence as low as 0.04% - 0.7%.;1 likely secondary to a paucity of lymphoid tissue in the breast. Breast lymphoma comprises primary breast lymphoma (PBL) and secondary breast lymphoma (SBL) and is challenging to diagnose given non-specific and overlapping imaging features with each other and other breast malignancies.2 Thus, imaging findings, appropriate clinical context, and biopsy are essential for diagnosis.
A rare disease, PBL accounts for fewer than 1% of breast malignancies and fewer than 2% of extranodal non-Hodgkin lymphomas (NHL).1,3 Initial diagnostic criteria for PBL, as proposed by Wiseman and Liao,4 are an adequate specimen with close proximity to breast parenchyma and lymphomatous infiltrate for pathologic examination, no prior diagnosis of extra-mammary lymphoma, and no evidence of concurrent widespread disease except for simultaneously appearing ipsilateral axillary lymph nodes. Updated additional criteria include ipsilateral supraclavicular lymph nodes equating to regional disease.5
Primary breast lymphoma is almost always NHL, predominantly a high-grade, B-cell lymphoma, with diffuse, large B-cell lymphoma being the most common type (45%–79%).1,3 Follicular lymphoma (15%), mucosa-associated lymphoid tissue lymphoma (12.2%), and Burkitt lymphoma (10.3%) have also been identified in the breast but have a lower prevalence.5
The PBL stage and subtype have a direct impact on prognosis. Stage I PBL (confined to the breast, no axillary lymph node involvement) has a 53.8% recurrence rate and a 15.4% mortality rate, and stage II PBL (involvement of axillary lymph nodes) has a 33.3% recurrence rate and a 33.3% mortality rate.5
Imaging of PBL
On mammography, PBL demonstrates a solitary oval or round mass with nonspecific margins usually circumscribed or indistinct. Rarely, spiculated margins are seen. A hyperdense appearance is the most common .6,7 Asymmetries and architectural distortion are infrequent findings. Calcifications are almost always absent.6,7. Masses are larger in PBL than in SBL, with a mean diameter of 2.3 – 4.6 cm.6
On sonography, PBL is seen as a solitary oval or irregularly shaped mass with nonspecific features, circumscribed to indistinct margins, predominantly hypoechoic and usually in a parallel orientation.6 Posterior acoustic enhancement with or without echogenic rim can be present7 and it is usually hypervascular on Doppler (55-64%).
On MRI, PBL usually presents as a mass with nonspecific features similar to those of breast adenocarcinoma.6 With18FFDG PET, PBL demonstrates high uptake, indistinguishable from any glucose-avid breast malignancy.6
CONCLUSION
Primary breast lymphoma has nonspecific imaging features and is prospectively indistinguishable from other breast malignancies at imaging alone. However, utilizing clinical context and implementing appropriate biopsy techniques to support imaging findings help to diagnose PBL.
References
- Giardini R, Piccolo C, Rilke F. Primary non-Hodgkin’s lymphomas of the female breast. Cancer. 1992;69(3): 725–735.
- Brogi E, Harris NL. Lymphomas of the breast: pathology and clinical behavior. Semin Oncol.1999;26(3):357–364.
- Duncan VE, Reddy VVB, Jhala NC, Chhieng DC, Jhala DN. Non-Hodgkin’s lymphoma of the breast: a review of 18 primary and secondary cases. Ann Diagn Pathol. 2006;10(3):144–148.
- Wiseman C, Liao KT. Primary lymphoma of the breast. Cancer. 1972;29(6):1705–1712. Raj SD, Shurafa M, Shah Z, Raj KM, Fishman MDC, Dialani V.Primary and Secondary Breast Lymphoma: Clinical, pathological and multimodality imaging review rg.2019180097Yang WT, Lane DL, Le-Petross HT, Abruzzo LV, Macapinlac HA. Breast lymphoma: imaging findings of 32 tumors in 27 patients. Radiology. 2007;245(3):692–702.Liberman L, Giess CS, Dershaw DD, Louie DC, Deutch BM. Non-Hodgkin lymphoma of the breast: imaging characteristics and correlation with histopathologic findings. Radiology. 1994;192(1):157–160.
References
Citation
N M, P K.Primary Breast Lymphoma . Appl Radiol. 2021; (4):47-49.
July 15, 2021