Undifferentiated Embryonal Sarcoma of the Liver
Images





CASE SUMMARIES
Case 1: A 4-year-old girl with prior history of congenital heart defects presented with lethargy, decreased appetite and intermittent fevers. On examination, a nontender mass was noted in the right upper quandrant.
Case 2: A 7-year-old boy with no medical history presented with abdominal mass, discomfort, nausea, lethargy and early satiety.
IMAGING FINDINGS
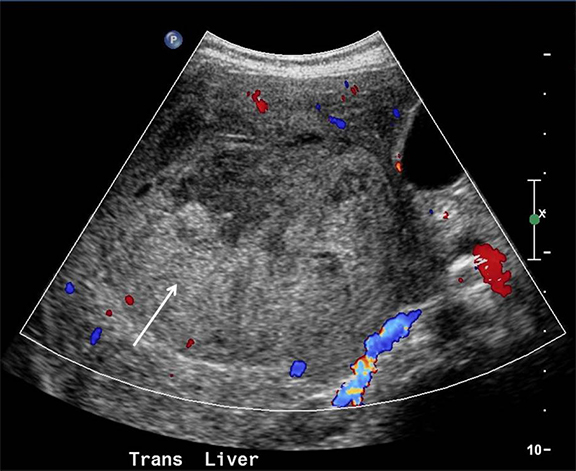
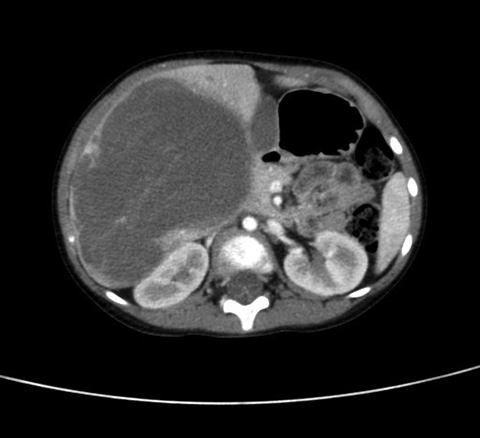
Case 1: Initial abdominal ultrasound scan demonstrated a large heterogeneous, echogenic mass within the liver displaying poor blood flow (Figure 1). A contrast-enhanced CT scan of the chest, abdomen and pelvis was then performed, revealing a well-defined, hypodense mass in the right lobe of the liver (Figure 2) measuring approximately 11.3 cm AP x 9.8 cm transverse x 9.2 cm in the sagittal plane. An arterial phase CT scan showed a hypodense mass with a hyperdense rim (Figure 3A) and a delayed venous phase scan showed the low-density mass with areas of increased density displaying the solid nature of the lesion (Figure 3A). These findings combined with biopsy confirmed undifferentiated embryonal sarcoma (UES).
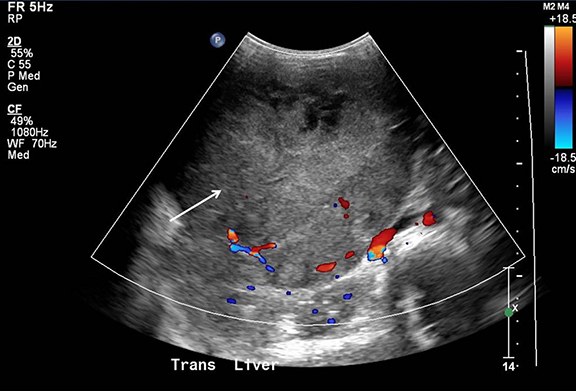
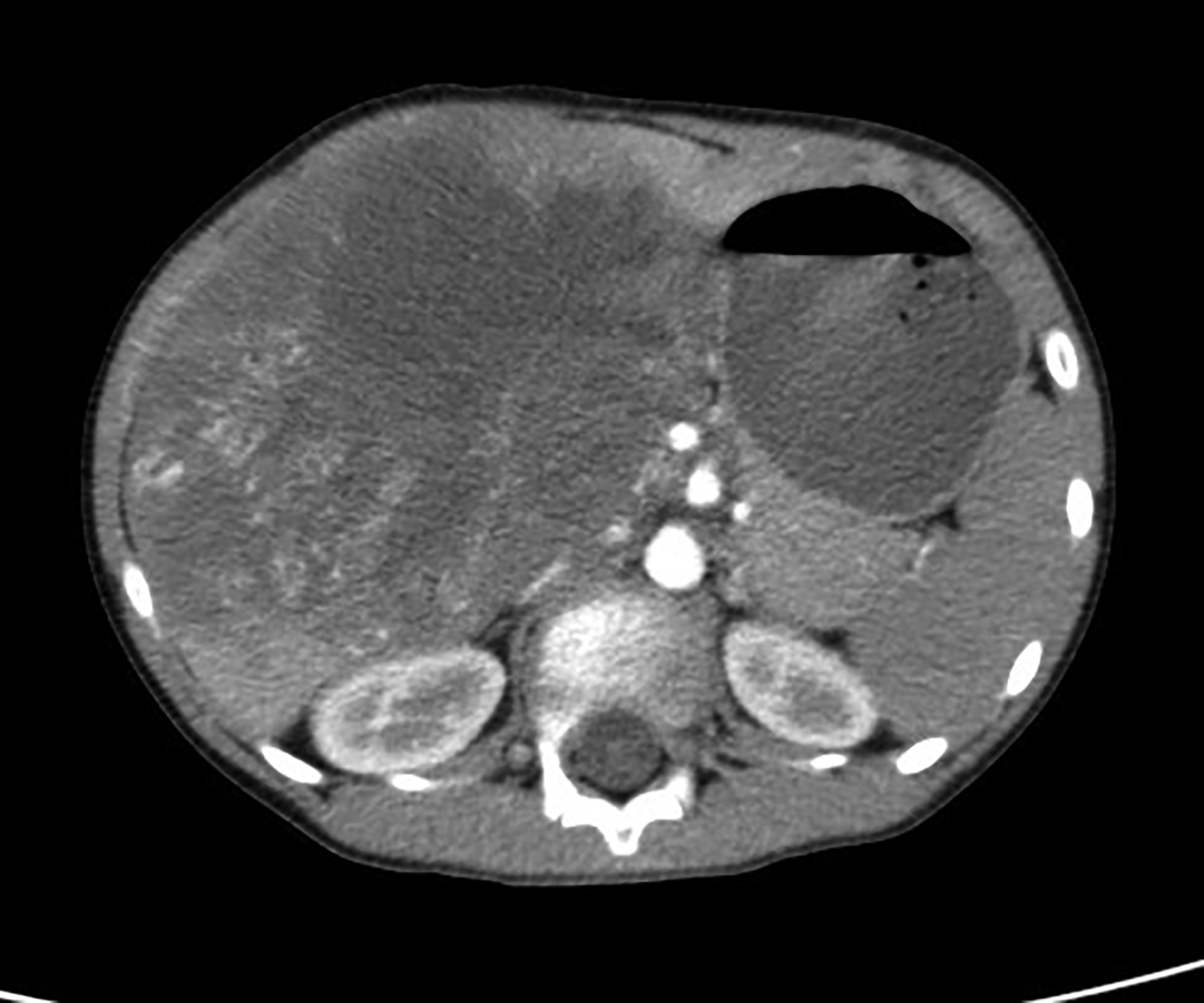
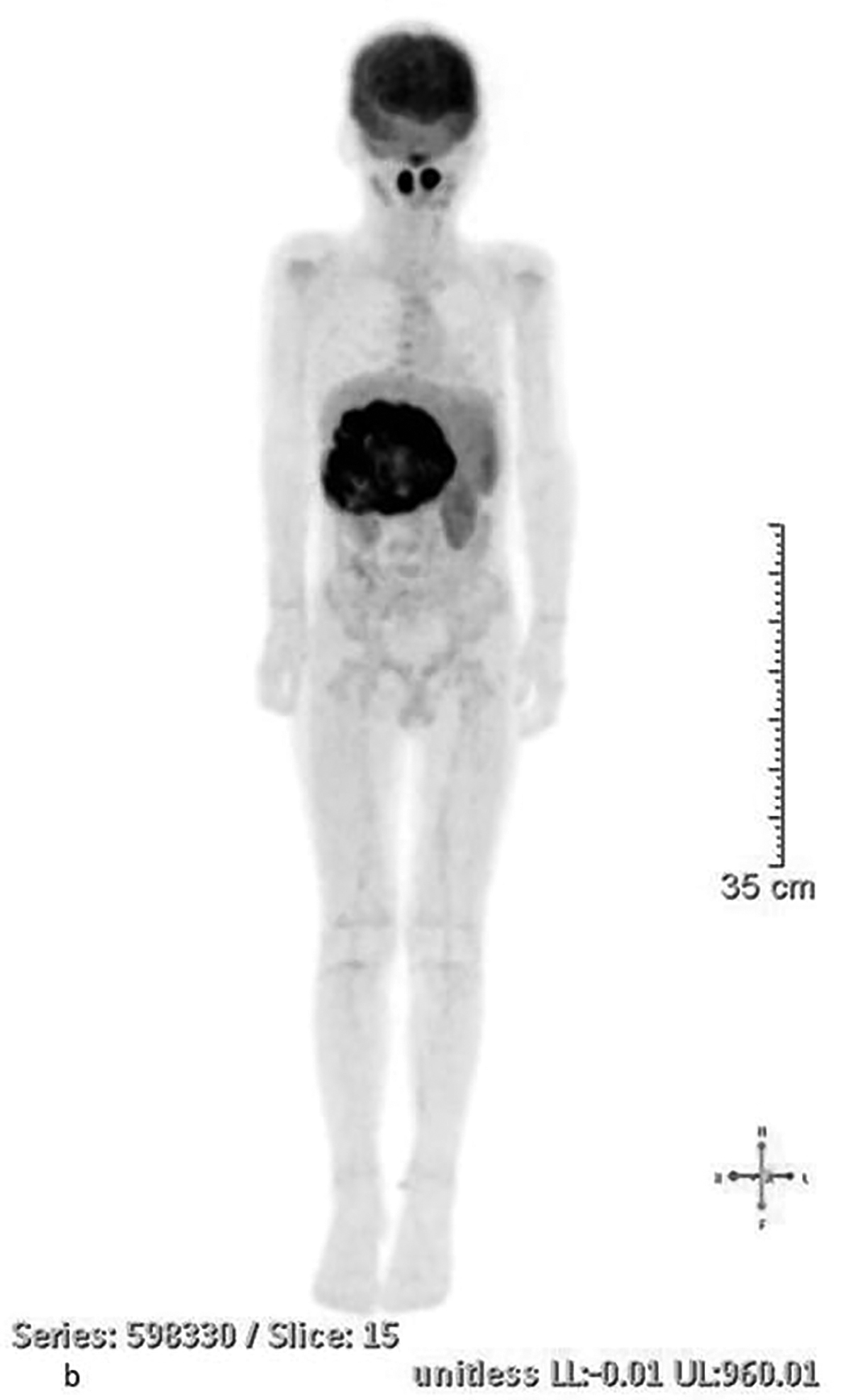
Case 2: An abdominal ultrasound scan initially revealed a large heterogeneous lesion in the center of the liver with a small amount of blood flow (Figure 4). Inconclusive ultrasound results warranted a CT scan of the chest, abdomen and pelvis with contrast, which showed a heterogeneous low-density lesion within the right lobe of the liver that extended to the left lobe (Figure 5). The mass measured approximately 12.3 AP x 12.3 transverse x 10.7 in the sagittal plane. Arterial-phase CT showed a well-defined hypodense mass with vessels coursing throughout (Figure 6A). Delayed venous phase demonstrated the solid consistency of the mass by showing continued filling in of the mass (Figure 6B). A PET scan was done to evaluate the extent of the disease. FDG-avid tissue was documented in the large lobulated hepatic mass (Figure 7A,7B).
DIAGNOSIS
Undifferentiated embryonal sarcoma of the liver.
Differential diagnoses include: hepatoblastoma, hepatocellular carcinoma, cystadenocarcinoma, hydatid cyst or atypical metastases.
DISCUSSION
Undifferentiated embryonal sarcoma (UES) of the liver is an uncommon primitive mesenchymal tumor occurring mainly in the pediatric population with a predominant age range of 6-10 yrs. Although rare, UES is the 3rd-most common cause of primary hepatic neoplasms in children after hepatoblastoma and hepatocellular carcinoma. The pathogenesis behind UES is not fully understood. However, it is hypothesized that UES is the malignant counterpart to mesenchymal hamartoma (MH). Various studies have shown MH and UES to have similar chromosome-19 abnormalities, specifically a translocation at 19q13.4.1 There are also reports of UES patients displaying germline p53 mutations linking UES to Li Fraumeni syndrome. Therefore, thorough family and genetic histories are important in aiding in this diagnosis.2
UES often presents as a right upper-quadrant abdominal mass with or without an association of pain, weight loss, fever, anorexia or other secondary symptoms. Tumor markers, such as alpha-fetoprotein and cancer antigen 125, are rarely elevated. UES is a rapidly growing aggressive tumor that can invade the inferior vena cava and right atrium and most often metastasize to the lungs and skeleton.3
UES is characterized as a solid tumor, most often in the right lobe of the liver, which grows rapidly, causing the development of cysts as a result of necrosis. On ultrasound UES typically appears as a well-defined heterogeneous echogenic hepatic mass with small anechoic areas. Computed tomography (CT) generally shows a well-defined, intrahepatic mass that is hypodense compared to surrounding parenchyma with various hyperdense septae and solid portions throughout. CT may also reveal a thin, dense rim surrounding the tumor, which on pathologic exam corresponds to a fibrous pseudocapsule. Comparison of pre- and postcontrast CT scans may show a more prominent low attenuated mass in the postcontrast phase.3 Using magnetic resonance imaging (MRI), UES appears as a hypointense and hyperintense signal on T1- and T2-weighted images, respectively. Contrast MRI often shows a heterogeneous enhancement of the mass, which is most prominent in the late portal venous phase.4 UES is often misdiagnosed as a cystic mass or hematoma based on the cystic appearance seen on CT and MRI. Overall, ultrasound gives a more accurate depiction of the solid tumor consistency and allows for a more precise differential diagnosis.
Ultimately, the diagnosis of UES requires a combination of clinical history, radiographic imaging and pathological examination. While immunohistochemistry can be key in confirming this diagnosis, tumor markers are rarely consistent from case to case. Most often tumor cells are positive for a1-antitrypsin and vimentin. Markers CK, CK19, actin, desmin, and CD56 are inconsistently positive.5
While UES is generally associated with a poor prognosis, early diagnosis and an aggressive multimodal treatment approach can significantly increase survival time. The ideal treatment includes complete surgical resection with negative margins. Since complete resection is not always feasible, surgical resection with neoadjuvant and adjuvant chemotherapy and radiation to sites of metastasis has improved mean survival time from 12 months to 52 months.2 A significant increase in survival time has been shown in patients who have undergone tumor resection followed by adjuvant transcatheter arterial chemoembolization. One study shows a tumor recurrence was delayed from 14 months to 30 months when transcatheter arterial chemoembolization was used.6 Orthopnoic liver transplant (OLT) has been successful as a therapeutic option for patients with unresectable tumors.4 18-fluorodeoxyglucose positron emission tomography/computed tomography is useful in staging, monitoring therapy and evaluation of recurrence.2
CONCLUSION
Undifferentiated embryonal sarcoma of the liver is a rare and highly aggressive primitive mesenchymal neoplasm that should be considered in pediatric patients presenting with a right upper quadrant mass and nonspecific constitutional symptoms. An early, accurate diagnosis and prompt introduction of treatment is directly related to a better prognosis and increased survival rate.
REFERENCES
- Putra, J., Ornvold, K. Undifferentiated Embryonal Sarcoma of the Liver: A Concise Review. Arch Pathol Lab Med. 2015;139:269–273.
- Plant, A., Busuttil, R., Abbas, R., et al. A Single-institution Retrospective Cases Series of Childhood Undifferentiated Embryonal Liver Sarcoma (UELS): Success of Combined Therapy and the Use of Orthotopic Liver Transplant. Journal of Pediatric Hematology/ Oncology. 2013; 35(6): 451-455.
- Moon, W., Kim, W., Kim, I., et al. Undifferentiated embryonal sarcoma of the liver: US and CT findings. Pediatric Radiology. 1994; 24: 500-503.
- Walther, A., Geller, J., Coots, A., Towbin, A., Nathan, J., Alonso, M., Sheridan, R., Tiao, G. Multimodal therapy including liver transplantation for hepatic undifferentiated embryonal sarcoma. Liver Transplantation. 2014; 20(2):191-9.
- Cao, Q., Ye, Z., Chen, S., et al. Undifferentiated embryonal sarcoma of liver: a multi-institutional experience with 9 cases. Int J Clin Exp Pathol. 2014; 7(12): 8647–8656.
- Li, X., Gong, S., Song, W., et al. Undifferentiated liver embryonal sarcoma in adults: A report of four cases and literature review. World J Gastroenterol. 2010;16(37): 4725–4732.
Citation
B K, S J, Towbin, R. Undifferentiated Embryonal Sarcoma of the Liver. Appl Radiol. 2015;(10):.
October 2, 2015