MRI suitable for trachelectomy treatment planning for cervical cancer patients
Radical trachelectomy is a fertility-preserving option for some women diagnosed with early-stage cervical cancer. Compared with radical hysterectomy, patients who have a trachelectomy tend to have fewer complications.
Magnetic resonance imaging (MRI) helps surgeons pre-operatively assess cervical cancer. MR images accurately show the size of the tumor, the presence of suspicious lymph nodes, and the involvement of the lower uterine segment/internal os (IO).
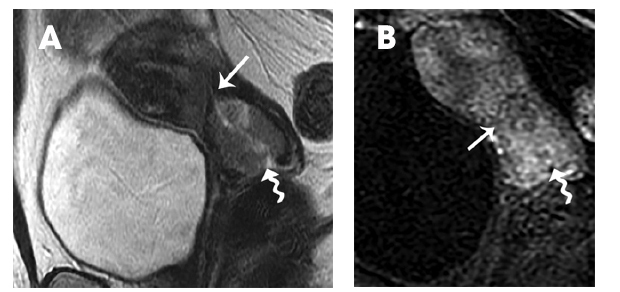
A 50-year-old woman with massive hemorrhage and cervical cancer. (A) Sagittal T2 weighted and (B) T1 weighed sequence show an endophytic mass in the cervix representing a squamous cell cancer (squiggly arrow) and involves the internal os (arrow).
Researchers at the University of Texas-MD Anderson Cancer Center conducted a study to determine how well MRI could detect tumor-free margins from the internal os. Specifically, they correlated the actual distance 5 millimeters or less or more than 5 millimeters from the tumor to the IO at MRI, and compared this with the distance measured at histopathology for 79 patients. Published in the June 2016 issue of Clinical Radiology, the study determined that its high specificity, accuracy, and negative predictive value (NPV) makes MRI suitable for treatment planning in candidates for trachelectomy.
Lead author Priya Bhosale, MD, an associate professor in the Department of Diagnostic Radiology, and colleagues identified 79 cervical cancer patients who had a contrast-enhanced MRI scan within three weeks of having a radical hysterectomy. Ppatients who had a radical hysterectomy were selected instead of patients who had a trachelectomy procedure because it would not have been feasible to measure the distance from the IO on pathology of trachelectomy specimens, according to the study authors.
Two radiologists specializing in gynecologic oncology reviewed the MRI scans. For each patient, they recorded tumor size and distance from the IO, and the presence or absence of adenopathy. Findings were categorized as positive if the tumor involved the IO, negative if it did not. A pathologist independently evaluated the tumor size, tumor involvement of the IO, and tumor distance from the IO on explanted specimens. Pathology results were considered the reference standard for assessing the accuracy of MRI images. In addition, a subset analysis was performed on 70 patients who might have qualified for a radical trachelectomy procedure.
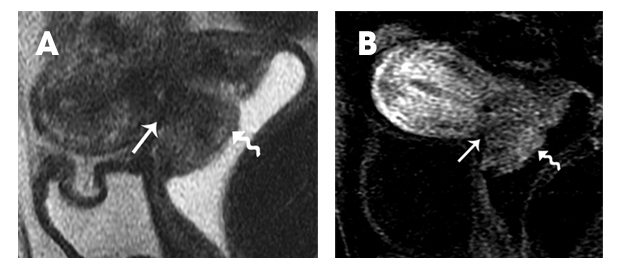
A 41-year-old woman with cervix cancer (A) Sagittal T2 weighted and (B) T1 weighed sequence show an endophytic mass in the cervix representing a squamous cell cancer (squiggly arrow) and involves the internal os (arrow).
The MRI images scans demonstrated high specificity for the subset cohort and the total cohort, at 93.2% and 93.8% respectively, for predicting involvement of the IO. The NPV was 96.5% and 95.3%. MRI had a specificity of 97.9% and 98.3% and a positive predictive value (PPV) of 94.7% for the subset cohort and 95% for the total cohort for the assessment of the distance from the IO.
“In other words, if MRI did not raise concern about IO involvement (less than or equal to 5 mm), it was unlikely that the pathology specimen would show IO involvement, and surgeons could proceed with the procedure with a very high likelihood of obtaining negative margins,” the authors wrote.
Tumor size at MRI and on gross pathology also had high correlation. The authors stated that it was reasonable to suggest that patients who had tumors greater than 2 cm on clinical exam and who desired fertility-sparing surgery should undergo preoperative MRI assessment for factors that could preclude surgical resection, such as IO involvement. However, they cautioned that while most patients can undergo a successful trachelectomy based on a clinical FIGO (International Federation of Gynecology and Obstetrics) stage, about one-fourth may need radical hysterectomy as a result of a positive resection margin, or post-trachelectomy chemoradiation for positive pelvic lymph nodes on final pathology.
REFERENCE
- Bhosale PR, Iyer RB, Ramalingam P, et al. Is MRI helpful in assessing the distance of the tumour from the internal os in patients with cervical cancer below FIGO Stage 1B2? Clinical Radiology 2016 71;6:515-522.
Citation
MRI suitable for trachelectomy treatment planning for cervical cancer patients. Appl Radiol.
May 24, 2016