MRI plus FET PET recommended for new glioblastoma cases
Images
The success of prolonged survival for a patient with glioblastoma is determined, in part, by the extent of the brain tumor’s surgical resection. German researchers suggest that contrast-enhanced magnetic resonance imaging (MRI) critically underestimates the metabolically active tumor volume of glioblastomas in some patients. In the March issue of the European Journal of Nuclear Medicine and Molecular Imaging, they recommend amino acid positron emission tomography (PET) scans for newly diagnosed patients
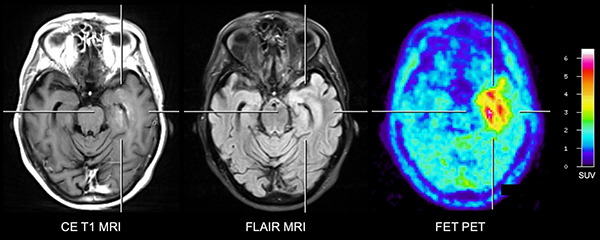
Contrast-enhanced (CE) MRI (left), fluid-attenuated inversion recovery (FLAIR) MRI (center) and FET PET (right). A considerable portion of FET PET tumor volume extends beyond the area of contrast-enhancement and is also partially located outside of areas of FLAIR hyperintensity.
Prior research correlating imaging studies with histopathological findings have shown that amino acid PET identified more of the extent of a tumor than contrast-enhanced MRI. Conducted by the Institute of NeuroScience and Medicine at Forschungszentrum Juelich and the Department of Neurology at University Hospital Cologne, the study of 50 newly diagnosed glioblastoma patients sought to determine volumetric differences between contrast enhancement on MRI and O-(2-[18F]fluoroethyl)-L-tyrosine (FET) accumulation on PET, and to compare them with fluid-attenuated inversion recover (FLAIR) on MRI. They evaluated tumor size, overlap, and spatial correlation.
Patients with neuropathologically confirmed untreated glioblastoma, initially had three-dimensional (3D) T2-weighted FLAIR MRI and 3D T1-weighted MRI scans. These were followed by a dynamic FET PET scan, performed on the same day for the majority of patients.
The researchers calculated tumor volume, spatial correlation, and the overlap between MRI-based and FET-based tumor volumes. They also visually recorded the differences between FET-based and FLAIR-based tumor volumes.
FET tumor volume was significantly larger than that seen on contrast-enhanced MRI for 43 cases, or 86%, at a mean of 21.5 mL and 9.4 mL respectively. No contrast enhancement was visible in 10 cases, and one showed no FET uptake. Spatial similarity between FET uptake and contrast enhancement was low and tumor overlap was moderate for the 40 cases showing increased FET uptake and contrast enhancement. Sixteen patients either showed no contrast enhancement or an overlap volume of less than 50% in combination with a low spatial similarity.
The researchers reported FET PET tumor volume was smaller than the FLAIR volume in 70% of patients, and similar in 20%. For the remaining 10%, a considerable portion of the FET PET tumor volume was outside the FLAIR volume.
“Considering that a maximally safe tumour resection is a critical component in the treatment of patients with GBM due to its survival benefits, adequate preoperative volumetric representation of the metabolically active tumour tissue is especially important,” wrote the authors. “Consequently, correct preoperative spatial delineation of the vital tumour tissue is essential for maximizing the extent of resection.”
REFERENCE
- Lohmann P, Stavrinou P, Lipke K, et al. FET PET reveals considerable spatial differences in tumour burden compared to conventional MRI in newly diagnosed glioblastoma. Eur J Nucl Med Mol Imaging. 2019;46(3):591-602.
Citation
MRI plus FET PET recommended for new glioblastoma cases. Appl Radiol.
March 8, 2019