Lung Cancer Screening Guidelines Perpetuate Disparities for Racial and Ethnic Minorities
 A new study in Radiology found that revised guidelines for lung cancer screening eligibility, made partly to address eligibility disparities, are perpetuating disparities for racial and ethnic minorities.
A new study in Radiology found that revised guidelines for lung cancer screening eligibility, made partly to address eligibility disparities, are perpetuating disparities for racial and ethnic minorities.
In 2014, the United States Preventive Services Task Force, an independent panel of medical experts, recommended lung cancer screening with low-dose chest CT in high-risk individuals to reduce cancer-related mortality. The initial eligibility guidelines had limitations, as they were derived from studies in which only 4% of participants were African American smokers.
In March 2021, the task force expanded eligibility, lowering the threshold for lung cancer screening eligibility from age 55 to 50 and from at least 30 to at least 20 pack-years of smoking. Pack-years are the number of packs smoked per day multiplied by the number of years smoking.
The revised guidelines, made partly to address eligibility disparities in screening, raised concerns over their continued reliance on age and pack-year thresholds.
“It was great to expand eligibility, but to just change the age and the pack-years doesn’t fully address lung cancer risk,” said Anand K. Narayan, M.D., Ph.D., radiologist and vice chair of equity in the Department of Radiology at the University of Wisconsin in Madison, and formerly of Massachusetts General Hospital (MGH) in Boston. “We’ve long known that some racial/ethnic minorities face a higher risk of lung cancer, and that level of risk is not adequately reflected in the new guidelines.”
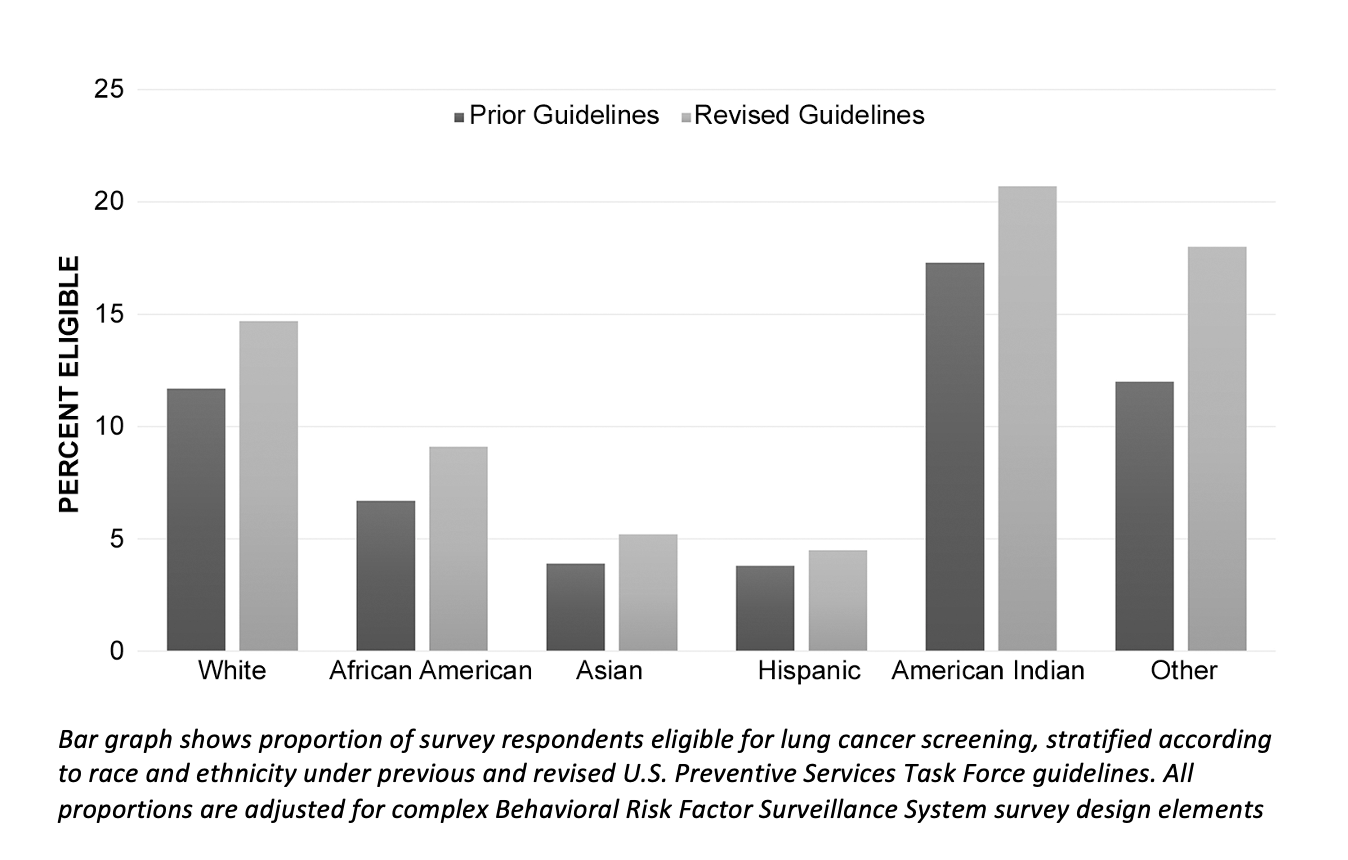
To learn more about the impact of the changes on disparities in lung cancer screening eligibility, Dr. Narayan, Divya N. Chowdhry, MD, a breast imaging radiologist at MGH, and colleagues looked at data from the 2019 Behavioral Risk Factor Surveillance System Survey, which included more than77,000 respondents. The survey results showed that the proportion of respondents eligible for lung cancer screening rose from 10.9% before the revisions to 13.7% after revisions. However, African Americans, Hispanics and Asian/Pacific Islanders remained less likely than whites to be eligible for screening. Under the new guidelines, 14.7% of whites were eligible for lung cancer screening, compared with 9.1% of African Americans, 4.5% of Hispanics and 5.2% of Asian/Pacific Islanders.
“Unfortunately, we saw no evidence that there was any change in the eligibility disparities for racial/ethnic minorities,” Dr. Narayan said. “Even though the new criteria were created in part to address the disparities, they don’t reflect the fact that racial/ethnic minorities are at higher risk.”
A better way to address the disparities, Dr. Narayan said, is through the incorporation of risk models into eligibility guidelines. Risk models can go beyond age and pack-years to include variables like family history and the presence of chronic obstructive pulmonary disease. Social determinants of health like employment, education status and food insecurity might also play a role.
“If we put social determinants of health into our model, then we can more accurately reflect risk,” Dr. Narayan said. “It can give us tools to direct our resources toward patients in terms of how much risk they are experiencing and how much care they actually need. We can then target high-risk patients for more intensive screening and diagnostic services.”
Dr. Narayan noted that in breast cancer screening, women are eligible for supplementary imaging with MRI if their lifetime risk of developing breast cancer is greater than 20%. A similar model could be employed in lung cancer screening, he said, potentially making more racial/ethnic minorities eligible for lung cancer screening.
“In a country that is so diverse and has patients in so many different circumstances, I feel as though we need new solutions to adequately reflect lung cancer risk for our patients and reduce lung cancer disparities in racial/ethnic minorities,” Dr. Narayan said.
Related Articles
Citation
Lung Cancer Screening Guidelines Perpetuate Disparities for Racial and Ethnic Minorities. Appl Radiol.
September 21, 2021