How We Do It | The Nasal Bridle: A Loop Retention Device
Images


The use of nasogastric (NG) and nasojejunal feeding tubes (NJ) has steadily increased over the past 20 years as they have become important approaches to providing adequate calories and hydration for children, older adults, and others who have temporary or long-term need for alternate pathways for nutrition.
Tube feeding can be an excellent option for any patient with a functional gastrointestinal tract, thereby avoiding intravenous hyperalimentation and its associated complications. Nasogastric and NJ feeding tubes are especially useful for nutritional supplementation for short-to-medium periods of time (<6 weeks) because they reduce the need for more invasive and expensive procedures, including surgical, endoscopic, or percutaneous gastrostomy or gastrojejunostomy.
After initial placement of a feeding tube, the main challenges are to maintain the tip of the feeding tube in a safe and effective position and to minimize inadvertent removal by the patient or staff. The target for tip position for an NG tube is generally within the gastric fundus, while the preferred tip position for an NJ tube is in at least the fourth portion of the duodenum to minimize the risk of fluid reflux into the stomach.
Historically, various types of taping and adhesive dressings were used to fix the feeding tube in position. Unfortunately, tube security with these dressings may be poor, and tubes are often inadvertently retracted into unsafe positions, such as in the esophagus for NG tubes or in the proximal duodenum or stomach for NJ tubes. They may also be prematurely removed entirely, necessitating a repeat placement. Replacing a feeding tube may require sedation or general anesthesia, especially in children, as well as additional radiation, particularly for NJ tube insertion where fluoroscopic guidance may be required.
The nasal bridle loop retention device (Applied Medical Technologies, Brecksville, Ohio) provides a more reliable method of securing a feeding tube for long periods of time.
Technique
Placing a nasal bridle requires neither imaging guidance nor sedation. The nasal bridle may be placed before or after the nasal tube; we prefer placing it after the NJ tube to prevent an unnecessary procedure if feeding tube insertion is unsuccessful. The child is placed in the supine position, and the procedure is performed as follows:
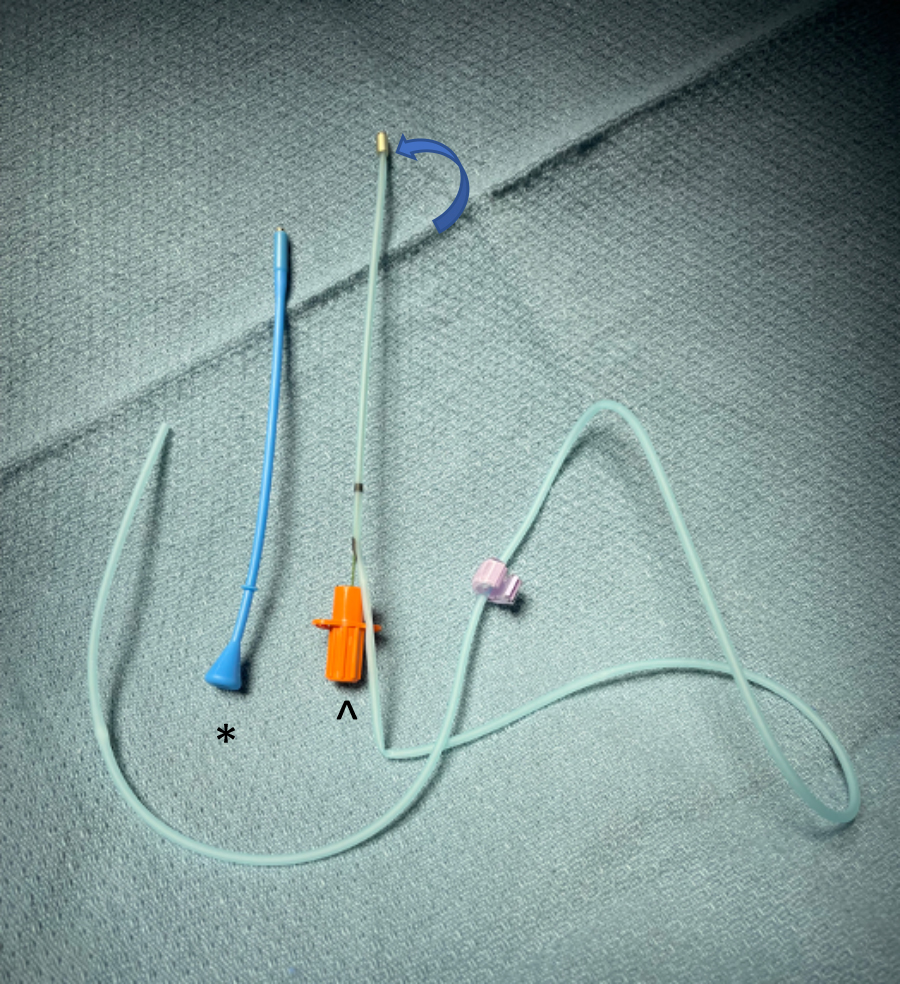
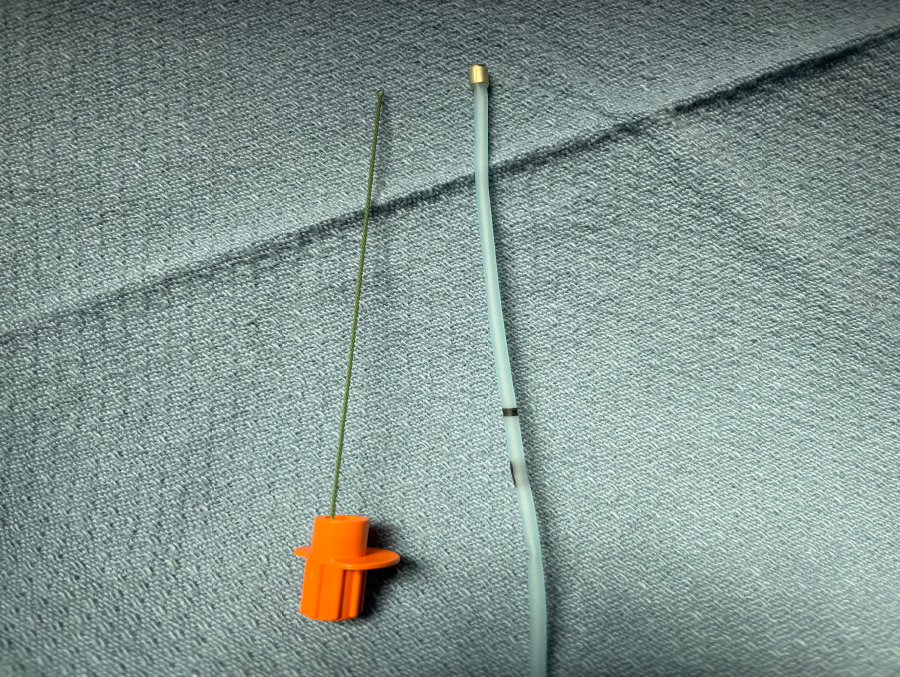
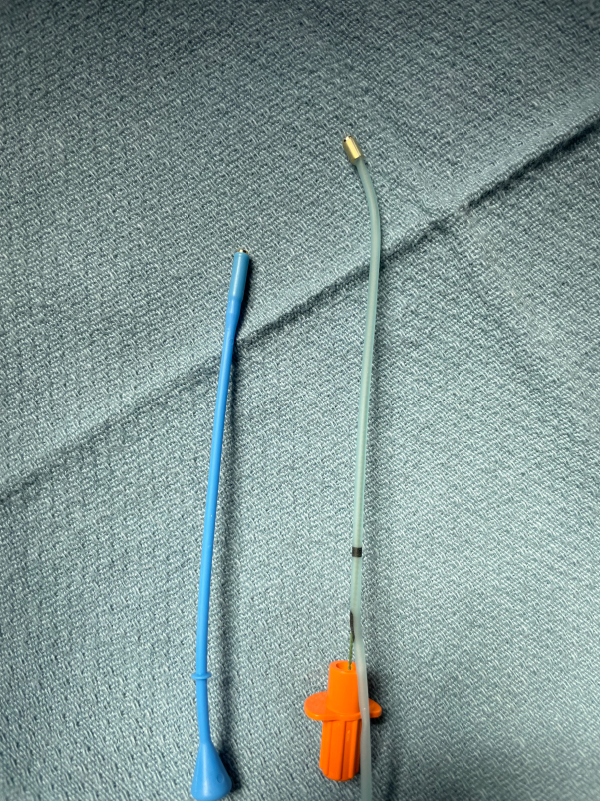
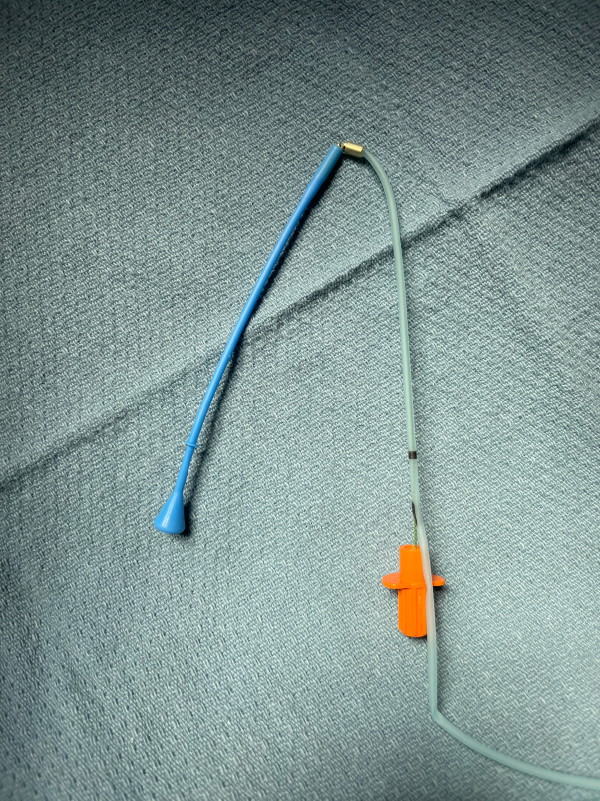
- The tips of the blue probe and catheter (Figure 1) with inner stylet are lubricated. The blue probe is inserted into the nostril opposite the feeding tube until the second ring is positioned at the bottom of the nostril (note: shorter depth is required for infants and small children). The probe and catheter are both directed posteriorly, not superiorly, in the nares, to extend posterior to the vomer bone.
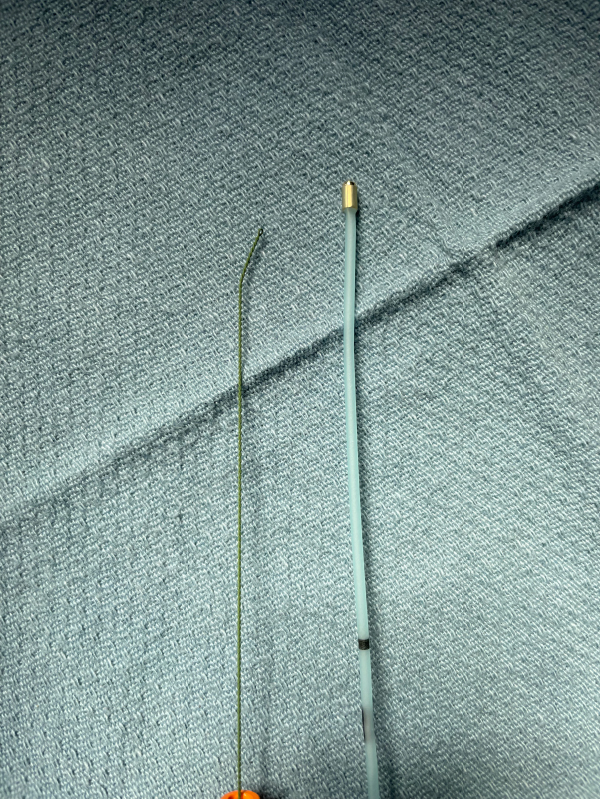
- The stiffening wire is gently bent into a hockey-stick shape and inserted into the bridle catheter, above the connection to the silicone tape and prior to placement in the nares (Figure 1). The shaping of the wire makes the bridle catheter directional if catheter manipulation is needed to find the magnetic tip of the probe. The catheter is inserted into the nostril with the feeding tube, tip directed to the midline, to approximate the magnets. If necessary, the orange stylet in the catheter should be pulled back about 1cm (1/2") until the magnets connect.
- A “click” will be felt when the magnets connect. Remove the stiffener from the bridle catheter.
- Slowly withdraw the blue probe and allow the catheter to advance through the nose, exiting the nares opposite the feeding tube. Continue until only the silicone tape remains in the nose, with each end exiting out one nostril. This creates a loop around the vomer bone (Figure 1).
- Cut the catheter portion from the silicone tape and discard the catheter and probe.
- Position the silicone tape adjacent to the feeding tube before closing a compression clip around both. The clip should be positioned approximately 1cm (1/2") from the nostril. Important: the clip should not contact the nostril as it may cause pressure necrosis (Figure 2).
- Once the clip is closed, a knot should be tied in the silicone tape just peripheral to the clip and the excess cut off.
Discussion
The nasal bridle loop retention system is technically easy to insert and usually takes less than 10 minutes, with most procedures completed in 5 minutes or less. Nasal bridle insertion is more invasive than securing an enteric feeding tube with tape or an adhesive product, and it does increase the cost of enteral feeding tube insertion.
However, the literature has shown that the incidence of dislodgement of taped NG tubes ranges from 43% to 82%. When NG tubes are secured with a bridle there is a 9-20% reduction in the incidence of dislodgement.1 The increased tube stability has several advantages, including significant cost reduction, shorter hospital stays, improved caloric intake, fewer radiographs for tube tip confirmation, and fewer complications. The improved tube security leads to a lower rate of untoward effects, including aspiration, as well as lower radiation exposure, more consistent delivery of calories, many fewer replacement procedures, and less escalation to more invasive procedures such as surgery, endoscopy, or percutaneous gastrostomy, gastrojejunostomy, and fundoplication.1 As is the case with any device, there are complications; the most common post-placement issues are epistaxis, nasal ulceration2,3 and skin injuries4 We have treated a child that developed pressure necrosis of the columella of the nasal septum (Figure 2).
Conclusion
The nasal bridle loop is an effective retention device for NG and NJ feeding tubes that reduces the frequency of tube malposition and loss. The improved tube security results in cost savings and reductions in potential complications and in the incidence of escalation to gastrostomy or gastrojejunostomy tube placement.
References
- Lavoie JA, Securing Nasogastric Tubes in Children. ProQuest Dissertation Publishing, 20. 28548981.
- Li AY, Rustad KC, Long C, et al. Reduced incidence of feeding tube dislodgement and missed feeds in burn patients with nasal bridle securement. Burns. 2018, 44:1203-1209. 10.1016/j.burns.2017.05.025.
- Brugnolli A, Ambrosi E, Canzan F, Saiani L: Securing of naso-gastric tubes in adult patients: a review. Int J Nurs Stud. 2014, 51:943-950 10.1016/j.ijnurstu.2013.12.002.
- Lynch A, Tang CS, Jeganathan LS, Rockey JG: A systematic review of the effectiveness and complications of using nasal bridles to secure nasoenteral feeding tubes. Aust J Otolaryngol. 2018, 1:8. 10.21037/ajo.2018.01.01.
Citation
. How We Do It | The Nasal Bridle: A Loop Retention Device. Appl Radiol.
March 8, 2022