Hook of the hamate fracture
Images




CASE SUMMARY
A 16-year-old boy presented with acute left wrist pain immediately after hitting a foul ball in a baseball game. The ball did not strike the patient’s wrist. Physical exam was notable for snuffbox tenderness and limited range of motion in all directions.
IMAGING FINDINGS
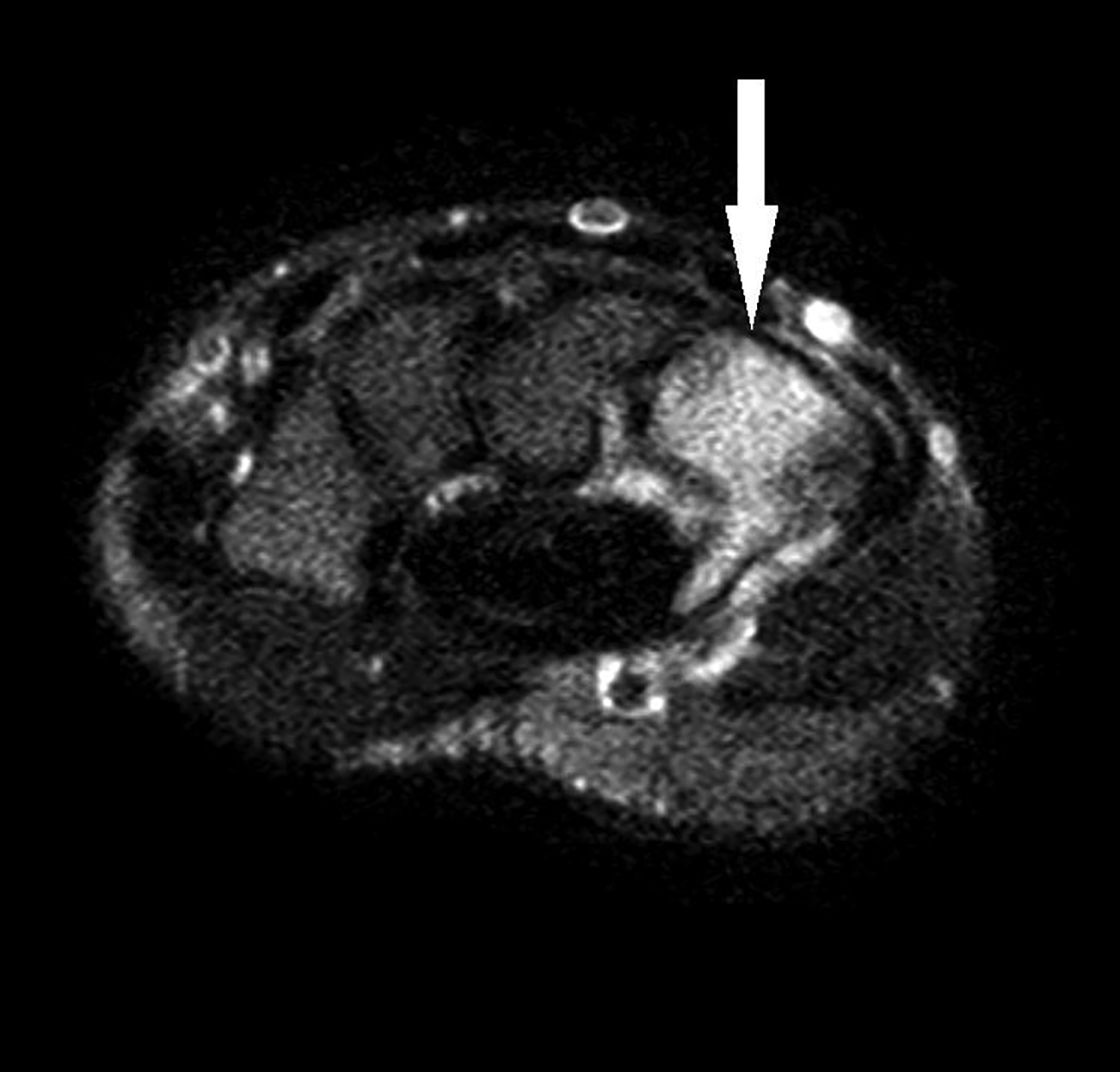
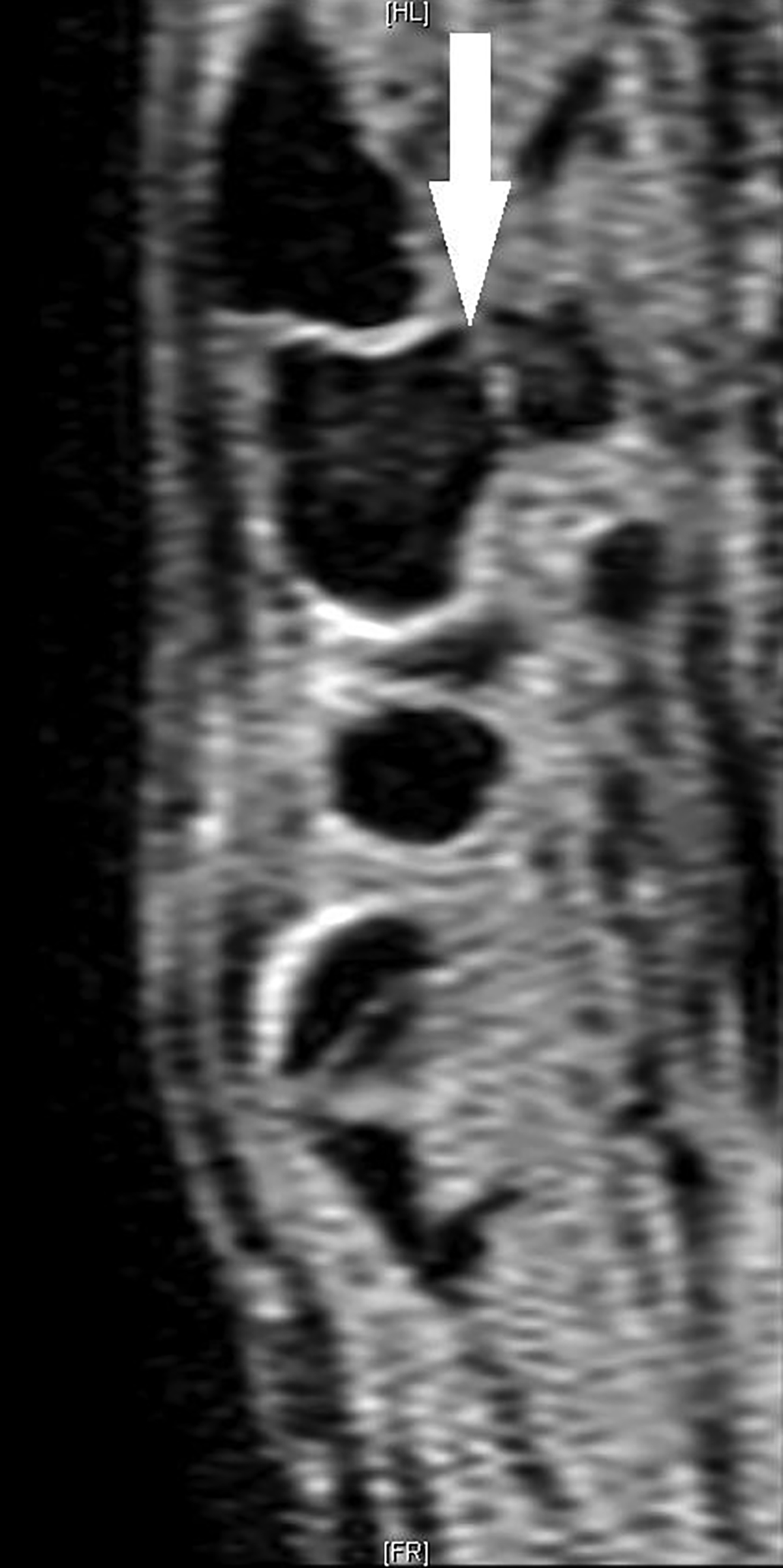
Initial plain radiographs of the left wrist were performed at an outside facility (Figure 1). AP and lateral views were negative for fracture, periosteal changes, soft tissue swelling or joint effusion. Because there was high suspicion for injury, an MRI was obtained. Axial T2-weighted images (Figure 2) demonstrate increased bone marrow signal within the hamate including the hook. Perihamate soft tissue edema is present. Coronal T1-weighted images (Figure 3) demonstrate decreased bone marrow signal within the hamate, including the hook. A sagittal T1 image (Figure 4) demonstrates abnormal linear signal through the base of the hook of the hamate consistent with a fracture. A sagittal WATS image (Figure 5) demonstrates abnormal linear signal through the base of the hook of the hamate consistent with a fracture. The scaphoid is normal on plain film and MRI.
DIAGNOSIS
Non-displaced fracture of the hook of the hamate.
The differential diagnosis includes scaphoid fracture (especially considering exam findings of snuffbox tenderness), other carpal bone fracture, ligamentous disruption without fracture, carpal bone dislocation.
DISCUSSION
Fractures of the hamate are rare and constitute approximately 2% of all carpal bone fractures.1 Fractures of the hamate are classified as those affecting the body and those affecting the hook. Fractures of the hook of the hamate are most commonly seen in male athletes that wield a bat or racket (ie, baseball, tennis, golf, and hockey players).2,4 Injury in athletes is thought to result from direct deforming force from the handle of the bat, racket, or club impinging on the hook of the hamate.2 Another common mechanism of injury is a fall on the outstretched hand, placing increased tension on the transverse carpal ligament thereby predisposing to an avulsion type fracture.3,4
The body of the hamate lies on the dorsoulnar aspect of the wrist, with its hook (a.k.a. hamulus) protruding volarly into the hypothenar eminence. The hook serves as a site of attachment of several structures including the flexor digiti minimi, opponens digiti minimi, pisiohamate ligaments, and distal portion of the transverse carpal ligament.5 On physical examination, patients typically present with chronic wrist pain and tenderness at the hypothenar eminence. Difficulty gripping things is common. A chronic hook of the hamate fracture that has been unrecognized and untreated may present as rupture of the 4th or 5th superficial or deep flexor tendon.5
Radiographic evidence and thus diagnosis of hamate fractures is difficult to recognize on standard AP and lateral imaging. There are three specialized radiographic views to bring the hamate into better view: the carpal tunnel view; the supinated oblique view with the wrist dorsiflexed; and the lateral view projected through the first web space with the thumb abducted. Note that these positions, especially the carpal tunnel views, may be difficult to achieve in patients with pain from acute injury.
If plain films are negative or there is a high clinical suspicion of fracture, CT or MRI may be indicated to evaluate for an occult fracture.5 Studies have shown CT to have a sensitivity of 100%, specificity of 94%, and accuracy of 97.2% in defining hook fractures, whereas plain radiographs have a 72% sensitivity, 88% specificity, and 80.5% accuracy.6 MRI is also sensitive for hamate fractures and is useful in detecting concomitant soft tissue injury.7 However, at this time there are no published sensitivity, specificity and accuracy data.
Non-displaced fractures of the hook of the hamate may be treated conservatively with casting and immobilization. For displaced fractures or chronic fractures of the hook, most surgeons will excise the fracture fragment to prevent partial or complete tendon rupture.5
CONCLUSION
Although rare, hook of the hamate fractures should be considered in athletes who develop acute wrist pain after swinging a bat, racket, or club. Exam findings of hypothenar tenderness and difficulty grasping should raise the clinician’s suspicion. Furthermore, although there are several specialized views to help visualize the hamate bone radiographically, negative plain films do not rule out acute fracture. CT has been shown to have superior diagnostic capability. MRI may be useful in detecting concomitant soft tissue and tendinous injury.
REFERENCES
- Botte M, Gelberman R. Fractures of the carpus, excluding scaphoid. Hand Clin.1987; 3:49-161.
- Stark H, Jobe F, Boyes J et al. Fracture of the hook of the hamate in athletes. JBJS. 1977; 59:575-582
- O’Shea K, Weiland A. Fractures of the hamate and pisiform bones. Hand Clin. 2012; 28:287-300.
- Binzer T, Carter P.Hook of the hamate fracture in athletes. Oper Tech Sports Med. 1996; 4:242.
- Green D, Wolfe S (2011) Green’s operative hand surgery, 6th edn. Elsevier/Churchill Livingstone, Philadelphia, PA.
- Andresen R, Radmer S, Sparmann M et al. Imaging of hamate bone fractures in conventional x-rays and high-resolution computed tomography: An in vitro study. Invest Radiol.1999; 34:46-50.
- Murthy N, Ringler M.MR imaging of carpal fractures. Magn Reson Imaging Clin N Am. 2015; 23:405-416.
Citation
J A, SA J, AJ T, R T.Hook of the hamate fracture. Appl Radiol. 2018; (2):29-31.
February 5, 2018