Gastric Wall Disruption in Blunt Abdominal Trauma
Images
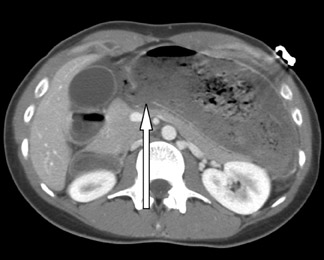
Blunt gastric rupture with subdiaphragmatic air, gastric dilatation, and posterior gastric wall disruption with evidence of stomach content extravasation
Findings
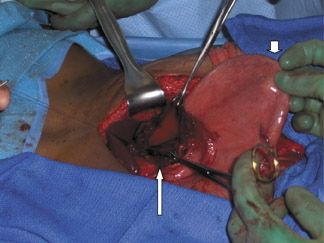
The CT scan of the abdomen and pelvis with intravenous contrast revealed a small focus of intraperitoneal gas anterior to the liver and a markedly dilated stomach filled with food. The posterior wall of the stomach was discontinuous with some spillage of gastric contents into the peritoneal cavity consistent with a gastric rupture (Figure 1). Upon return from CT scan, the patient continued to vomit, despite placement of a nasogastric tube. At laparotomy, there was murky, foul-smelling fluid present. Upon exploration, there was discoloration and fibrinous exudate along the anterior aspect of the lesser curvature of the stomach. The lesser sac was entered and the posterior stomach was inspected. There was gross spillage of gastric contents from a 6 cm perforation along the lesser curvature of the stomach (Figure 2). The gastric rent was approximately 10 cm in length after adequate debridement. The defect was closed in 2 layers using a continuous 3-0 VICRYL (Ethicon Inc., New Brunswick, NJ) full-thickness suture for the inner layer, and 3-0 silk, interrupted, seromuscular sutures for the outer layer. The patient was extubated postoperatively. She was discharged from the hospital on the seventh postoperative day in good condition.
Discussion
Blunt gastric rupture is an uncommon entity, occurring with an incidence of 0.02% to 1.7% in blunt abdominal trauma.1,2,3 Concomitant intra-abdominal injuries contribute to a significant morbidity and mortality. Prompt and accurate diagnosis is essential to early treatment.
Motor vehicle collisions are the most common cause of gastric rupture in blunt trauma, accounting for approximately 75% of cases.1,2 Other mechanisms include automobile vs. pedestrian, falls, assaults, and cardiopulmonary resuscitation.3 A history of consuming a recent meal is common with this injury, as a distended stomach is less pliable and more likely to rupture from blunt force.1,2
The majority of patients with gastric rupture will present with signs of shock or abdominal tenderness. However, as in this case, there may be scant signs of an acute abdomen if the rupture is initially contained within the lesser sac. Preoperative diagnosis may be difficult, because no physical signs are specific for gastric rupture. Although upright chest X-rays can diagnose free intraperitoneal air, chest X-ray fails to identify pneumoperitoneum in a substantial amount of patients with gastric rupture because most trauma chest films are done supine.1,4 Even so, only 50% to 66% of the gastric rupture cases develop enough free air to be detected by upright chest X-ray.1,4 Diagnostic peritoneal lavage can aid in the diagnosis when blood, food particles, or turbid or bilious fluid is aspirated.3 In the hemodynamically stable patient, the diagnostic study of choice is CT scan. CT scan can lead to early diagnosis of gastric rupture, and is accurate in detecting associated bowel, vascular, or solid organ injury prior to surgery.2
Optimal CT technique is essential for the diagnosis of many traumatic gastrointestinal lesions. The CT finding of disruption of the posteriorgastric wall has rarely been described in the literature but was diagnostic for this isolated injury preoperatively. At the time of this writing at our institution, CT for blunt abdominal trauma was performed after IV administration of contrast material and 500 mL of water as oral contrast. Intravenously, 125 mL of 68% iodinated contrast material was administered as a sustained bolus at 4 mL/sec, after which dynamic helical scans (LightSpeed, GE Healthcare, Chalfont St. Giles, U.K.) were obtained at 5 mm thickness and 5 cm intervals throughout the abdomen and pelvis with reconstructions at 2.5 cm. CT findings suggestive of gastric rupture include stomach dilatation, free intraperitoneal air, intraperitoneal position of the nasogastric tube, intraperitoneal fluid collection, and extraluminal oral contrast.2,5 In our patient, CT scan informed the diagnosis by showing free intraperitoneal air and disruption of the posterior wall with extraluminal gastric contents.
Most series report that the anterior wall of the stomach is the most common site of rupture, followed by the greater curvature, the lesser curvature, and the posterior wall.1 In our patient, the rupture was found on the posterior wall of the stomach. The rapid deceleration likely created a shearing force along the relatively fixed lesser curvature and the momentum of the massively distended stomach.1,2
Adequate debridement is necessary prior to repair. Repair of the stomach with a 2-layer closure is the treatment of choice for blunt gastric rupture.2 Many blunt injuries may require resection after debridement. Nasogastric drainage and thorough peritoneal lavage with saline are necessary after the injury is repaired.
Most complications are a result of the massive intraperitoneal contamination that ensues after rupture of a distended stomach and usually account for the late mortality.1,2 The most common complications are intra-abdominal abscess, gastric fistula formation, and wound infection.1,2,4 The mortality rate associated with gastric rupture is <66%.1,4 The high morbidity and mortality associated with this injury are related to thenumber of associated injuries, delay in diagnosis, and development of complications.4 Having a high index of suspicion, making an early diagnosis, performing adequate debridement and repair, and aggressively treating any complications are keys to survival in patients that have sustained a gastric rupture from blunt abdominal trauma.
Conclusion
We report a case of posterior gastric rupture following blunt abdominal trauma with CT findings of free intraperitoneal air and disruption of the posterior wall with leakage of gastric contents. These CT findings aided in early diagnosis of this uncommon injury. Although rare, gastric rupture is associated with a high morbidity and mortality. Early diagnosis and aggressive treatment with debridement, primary repair, andperitoneal lavage can help decrease intraperitoneal contamination. These elements are essential for successful outcomes in these patients.
- Brunsting LA, Morton JH. Gastric rupture from blunt abdominal trauma. J Trauma. 1987;27:887-891.
- Ishikawa K, Ueda Y, Sonoda K, Yamamoto A, Hisadome T. Multiple gastric ruptures caused by blunt abdominal trauma: Report of a case. Surg Today. 2002;32:1000-1003.
- Bruscagin V, Coimbra R, Rasslan S, et al. Blunt gastric injury. A multicentre experience. Injury. 2001;32:761-754.
- Courcy PA, Soderstrom C, Brotman S. Gastric rupture from blunt trauma. A plea for minimal diagnostics and early surgery. Am Surg. 1984;50:424-427.
- Takabe K, Ohtani T, Muto I, et al. Computed tomography findings of gastric rupture after blunt trauma. Hepatogastroenterology. 2000;47:901-903.