Fibromyxoid Sarcoma
Low-grade fibromyxoid sarcoma (LGFMS) is a rare, low-grade malignant neoplasm that usually develops in the proximal extremities and trunk and typically presents in younger adults. Local recurrence and metastases are common in adults and rare in children. CT, ultrasound, and MRI findings are useful in identifying tumor burden and determining the presence and extent of metastasis. Histopathologic examination and genetic/protein analysis are necessary to diagnose LGFMS. Expression of MUC4 and presence of the FUS/CREB3L2 fusion gene are key markers. Surgical resection with negative margins is the most effective way to prevent recurrence and metastasis.
Keywords: neoplasm, upper extremity, Musculoskeletal
Case Summary
A teenage male presented with a lump in the 4th web space of the left hand. The lump was firm but not tender or painful although it caused discomfort when gripping objects.
Image Findings
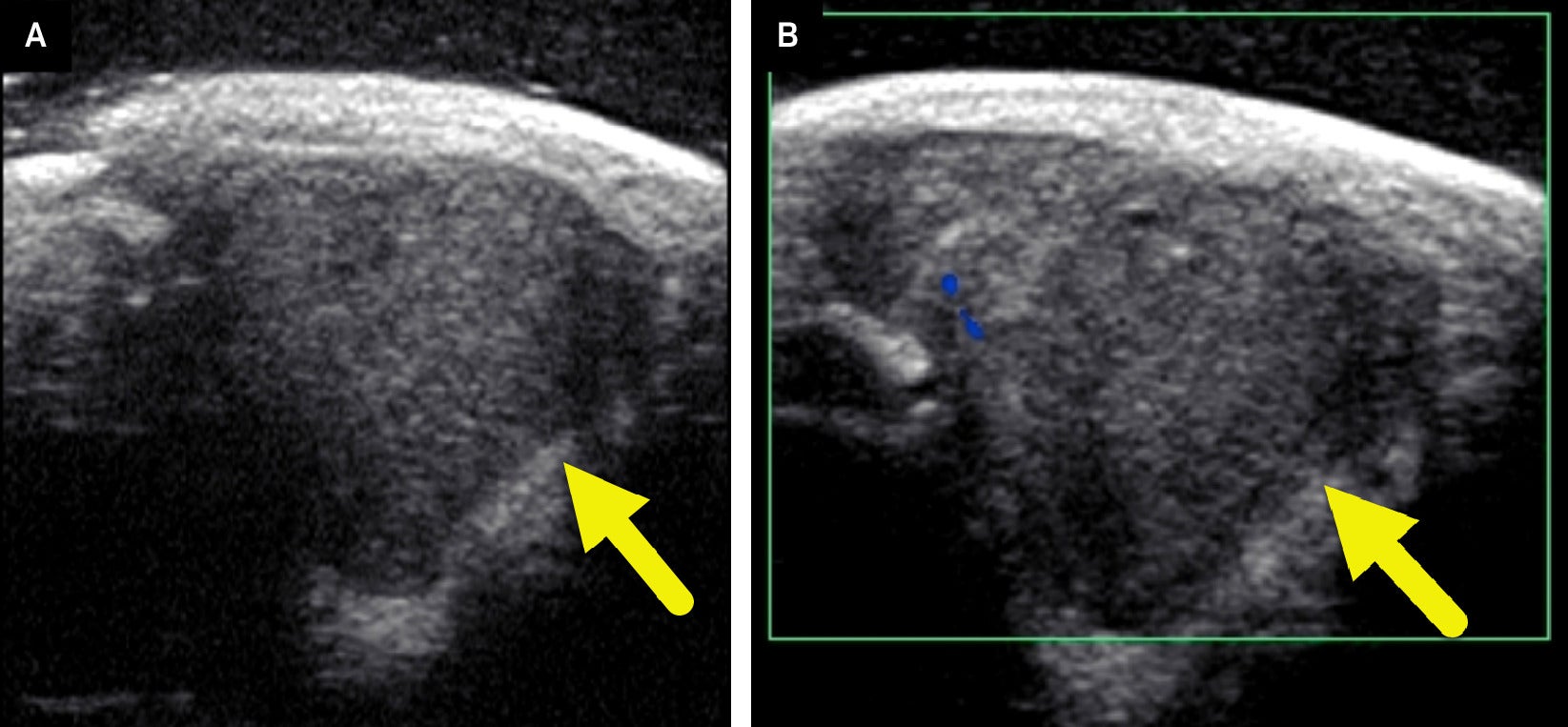
A radiograph of the left hand ( Figure 1 ) revealed a soft tissue mass in the web space between the ring and small fingers. No osseous abnormalities were noted. Ultrasound (US) ( Figure 2 ) demonstrated a well-circumscribed, hypoechoic soft tissue mass measuring 1.4×1.3×1.6 cm. No internal vascularity was noted.
Magnified radiograph of the hand shows a soft tissue mass (arrow) in the web space between the ring and small fingers. A small amount of relatively lucent fat is present on the more proximal aspect of the tumor.

(A) US of the soft tissue mass shows a solid hypoechoic lesion (arrow) at the area of concern. There is a small amount of echogenic fat along the lateral and deep margins of the tumor. (B) Color Doppler US shows minimal internal Doppler flow.
Diagnosis
Low-grade fibromyxoid sarcoma (LGFMS) confirmed by an excisional biopsy.
Differential diagnoses include hyalinizing spindle cell tumor with giant rosettes, soft tissue perineurioma, Ewing sarcoma, and tenosynovial giant cell tumor.
Discussion
LGFMS is a rare tumor primarily found in younger and middle-aged adults.1, 2 About 20% of cases are in children less than 18 years old. They commonly occur in the proximal extremities or trunk. However, almost any region of the body can be affected.2 LGFMS occurs slightly more commonly in males (M:F, 57:43).3 Although the tumor follows an indolent course, local recurrence is common and metastasis may occur, especially to the lungs.2
Children with LGFMS have a better prognosis than adults due to a decreased incidence of metastasis.2 A study of 31 patients under age 21 years had a 5-year local-relapse-free survival of 76±17.6% (95% CI) and a 5-year overall survival of 100%, with one case of metastasis.2 In comparison, a case series with 33 mostly adult patients had 64% local recurrence, 45% metastasis, and 58% overall survival.3 This variation may represent a difference in tumor biology.2
Radiographically, LGFMS appears as a noncalcified soft-tissue mass without adjacent bone erosion or destruction ( Figure 1 ).4 It is a solid hypoechoic mass on US with a more hypoechoic rim.4 It may have regions of nodularity and minimal internal blood flow on color Doppler ( Figure 2 ).4 The tumor is heterogeneous on CT, with heterogeneous enhancement and hypodense relative to muscle.4, 5 On MRI, the mass is hypo- to isointense compared with muscle on T1-weighted images and heterogeneous on T2-weighted images.5 It enhances heterogeneously after the administration of contrast media. Peritumoral edema is common.5 When an LGFMS is located within an intramuscular compartment, the “split fat” sign may be present.5 This finding is present when a rim of fat surrounds the tumor. The tumor may also have a gyriform pattern on T2-weighted or post-contrast sequences.4
As the name implies, LGFMS contains both myxoid and fibrous regions at histology.6 The tumor is comprised of fibroblastic spindle cells growing in a swirling pattern.6 The tumors have minimal cellularity and mitoses.6 Genetic analysis of LGFMS commonly reveals fusion of FUS-CREB3L2, making it a specific marker for the disease.7 Expression of the mucin four gene (MUC4) is also a highly sensitive and specific marker for LGFMS.8, 10
Surgical resection is the treatment of choice for LGFMS.2 The R classification system is used to define the absence or presence of tumor after treatment.9 R0 indicates complete remission, while R1 indicates microscopic residual tumor.9 The 5-year local recurrence-free survival is better for R0 disease compared with R1 disease (82.4% vs 53.6% in pediatrics).2 Data on the usefulness of chemotherapy or radiation therapy in LGFMS are virtually nonexistent, although it is expected to be ineffective given the low rate of mitosis.2
Conclusion
LGFMS is a rare, low-grade malignant neoplasm that usually develops in the proximal extremities and trunk and typically presents in younger adults. Local recurrence and metastases are common in adults and rare in children. CT, US, and MRI findings are useful in identifying tumor burden and determining the presence and extent of metastasis. Histopathologic examination and genetic/protein analysis are necessary to diagnose LGFMS. Expression of MUC4 and presence of the FUS/CREB3L2 fusion gene are key markers. Surgical resection with negative margins is the most effective way to prevent recurrence and metastasis.
References
Citation
Tsiouplis NJ, Towbin ;RB, Schaefer ;CM, Morgan ;D, Towbin ;AJ, ;4*. Fibromyxoid Sarcoma. Appl Radiol. 2025;(1):.
doi:10.37549/JPCR-25-0006
September 1, 2025