Endovascular Retrieval of Transthoracic Right Atrial Catheter Fragment
Images

Case Summary
An infant with Trisomy 21 underwent surgical repair of a large membranous ventricular septal defect (VSD). During surgery, the anesthesiologist noted difficulty intubating beyond the cricoid cartilage. Ultimately, intubation was performed using a 3.0 mm endotracheal tube without inflating the cuff. Postoperatively, the hospital course was complicated by a chylous pericardial effusion and multiple episodes of respiratory failure requiring bronchoscopy-assisted intubation. At the time of bronchoscopy, a tracheal ring was identified and subsequently treated with a tracheoplasty.
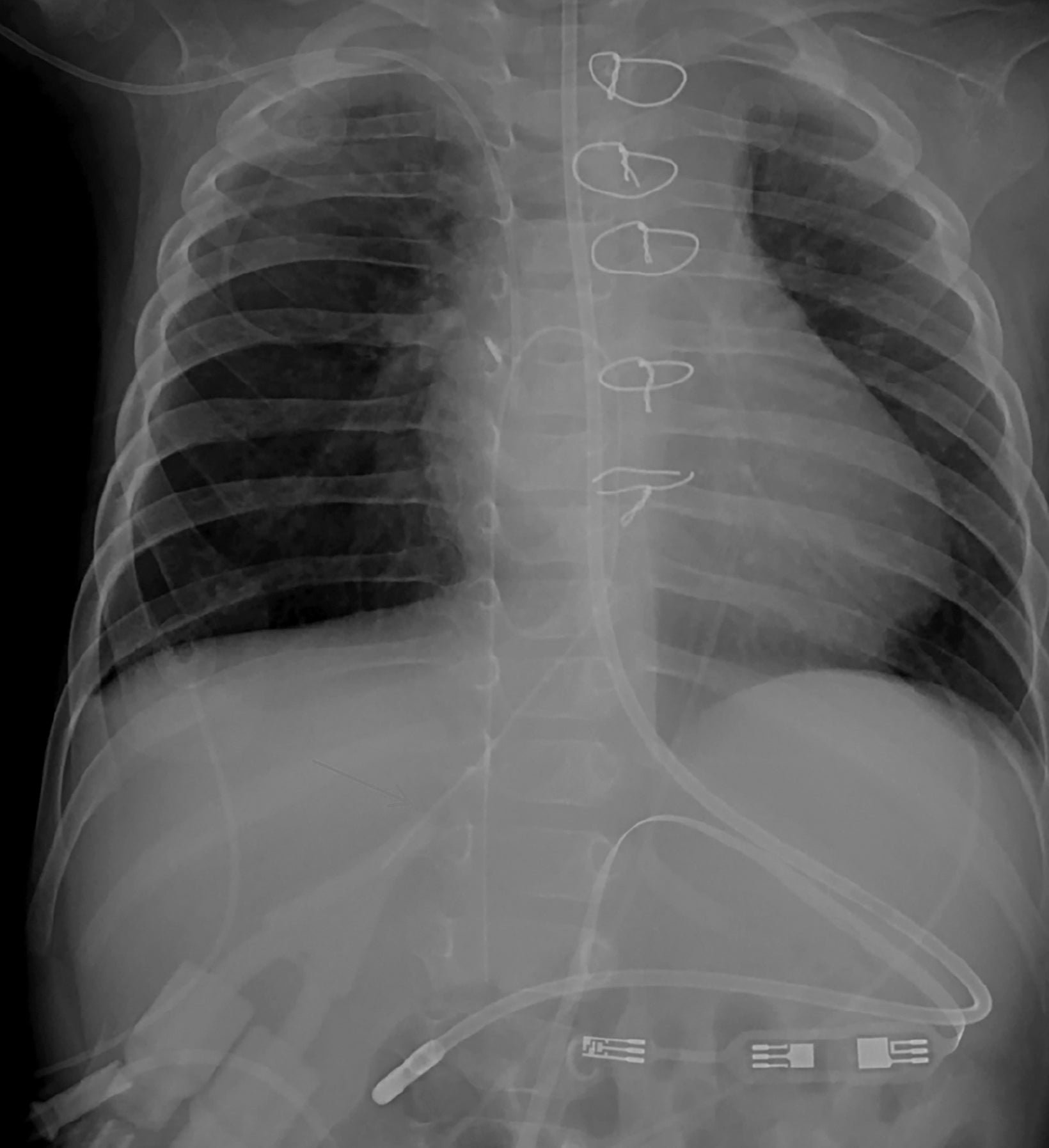
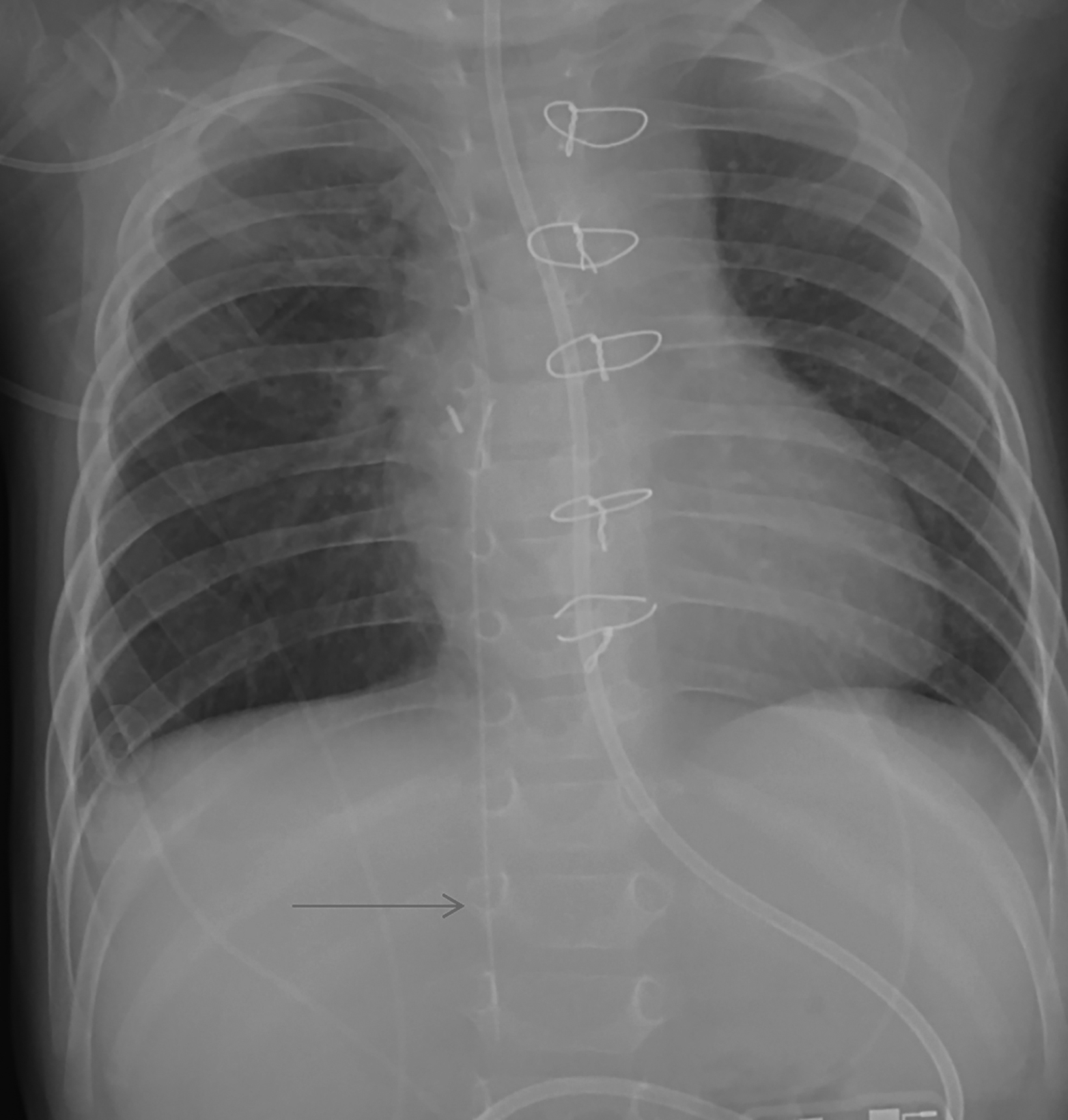
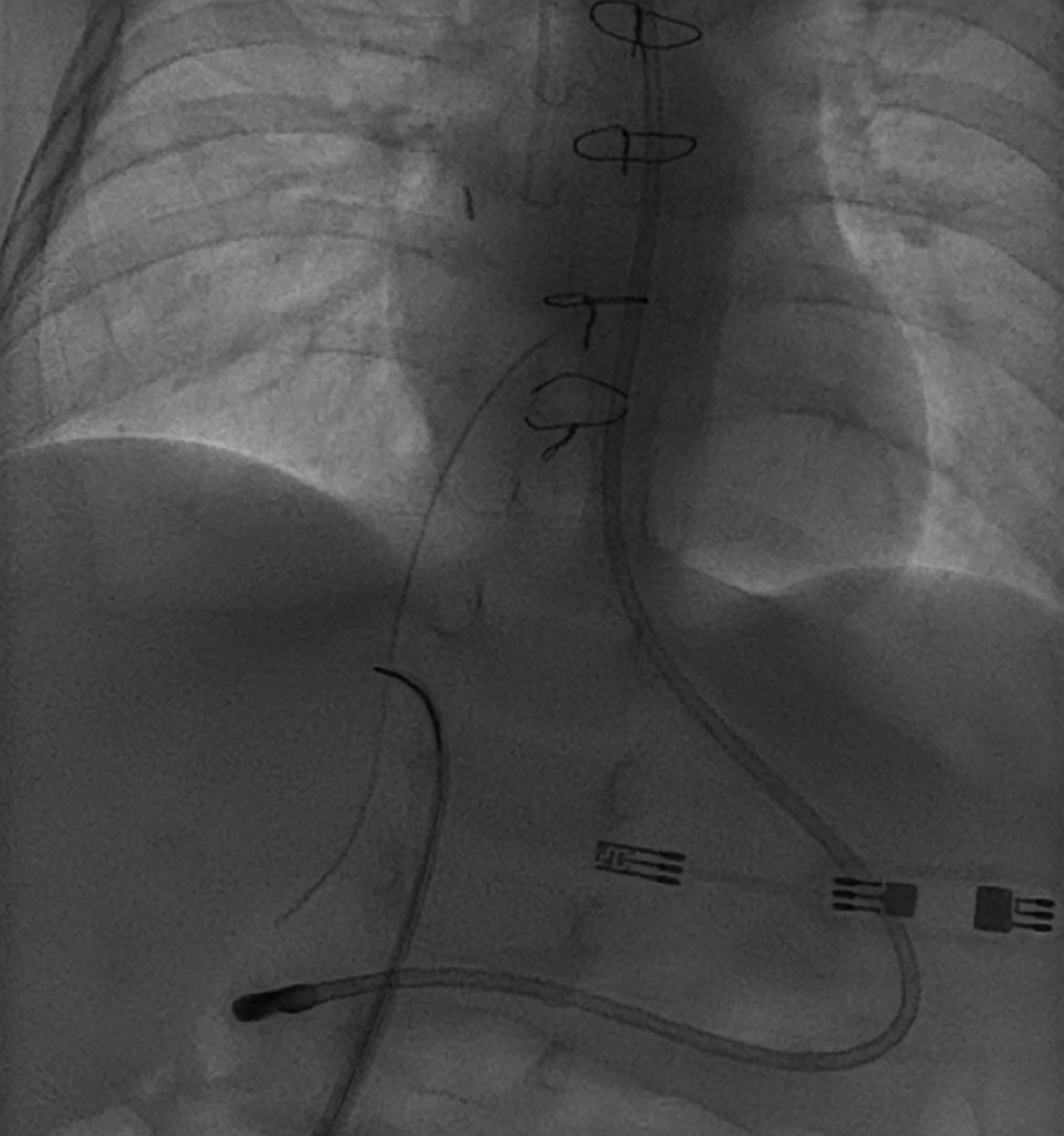
While the patient was on cardiopulmonary bypass, a 5-French dual lumen transthoracic right atrial catheter was placed. The catheter was secured with a purse-string prolene suture at the right atrial insertion site, as well as a silk suture at the skin exit site. Seven weeks later, the catheter was removed at the bedside. It was immediately noted the catheter had fractured and a long, retained catheter fragment was seen on a post procedural chest radiograph (Figure 1). The retained fragment was subsequently removed with a fluoroscopically guided endovascular snare (Figure 2).
Imaging Findings
A postoperative chest radiograph demonstrated a right atrial catheter with its tip coursing into the common hepatic vein. On a chest radiograph performed after catheter removal, a residual catheter fragment was seen with its tip in the inferior vena cava (Figure 1). Endovascular retrieval with a loop-snare device was successfully performed (Figure 2). Post-retrieval venography demonstrated no extravasation or vascular injury.
Diagnosis
Retained fragment of a transthoracic right atrial catheter. Differential diagnosis includes right atrial pacing wire, migration of peripherally inserted central catheter fragment into right atrium.
Discussion
Children requiring long-term central venous access present a challenge for clinicians, who must weigh concerns of complications such as venous thrombosis, infection, and catheter malfunction. In addition, in children with congenital heart abnormalities, the need for venous access must be balanced with the necessity for venous conservation for drug therapy and laboratory studies, and to preserve options for future corrective surgery, such as a superior vena cava to pulmonary artery (Glenn) shunt.1,2 Alternatives to upper- or lower-extremity venous access have been well described in the literature. They include transhepatic access, trans-lumbar access, and direct puncture into the brachiocephalic, intercostal, or other collateral veins.3
Though far less frequent, direct insertion of a central venous catheter into the right atrium is an attractive option in patients undergoing thoracic surgical procedures, especially those with limited central venous access. Venous conservation is especially important in children who require long-term parenteral nutrition or who are candidates for organ transplant.4,5
Initial experience with direct catheter placement into the right atrium was reported approximately 40 years ago.6 In our institution, intracardiac catheters are placed only at the time of open-heart surgery and are secured to the right atrium with a purse-string suture and to the skin using a non-absorbable suture. Catheters are removed at the bedside using gentle traction, without specific methodology to prevent bleeding or catheter fracture.
Several studies have examined the feasibility and safety of transthoracic intracardiac catheters. A large series evaluating placement of 523 such catheters in 351 patients found a high rate of bleeding (36.7%) with catheter removal, including hemodynamic compromise in 2.6% of patients.7 Another large study evaluated 1404 intracardiac central catheters inserted in 1118 patients. Of these, 8 patients (0.6%) required intervention for life-threatening bleeding, 6 because of line migration and 2 after catheter removal.8 Kumar, et al, found that catheter migration was less likely with patients having upper transthoracic insertion (above suprasternal notch) as opposed to lower insertion (inserted below diaphragm).9
Conclusion
Long-term central venous access in infants for drug infusion or parenteral nutrition, or in those with chronic conditions may require alternatives to routine extremity venous access. Direct intracardiac catheter insertion has been described, particularly via transthoracic approach, as an alternative for access in these patients. While RA catheter use is infrequent in the general population, it is often used postoperatively in children with congenital heart disease. Studies have documented several risks associated with intracardiac catheter use, particularly development of bleeding after catheter removal and catheter fracture. Retained fragments of catheter fractures can be removed using a transvenous, fluoroscopically guided endovascular snare.
References
- Stein ML, Quinonez LG, DiNardo JA, Brown ML. Complications of transthoracic intracardiac and central venous lines in neonates undergoing cardiac surgery. Pediatr Cardiol. 2019 Apr;40(4):733-737.
- Beham K, Dave H, Kelly J, Frey B, Hug MI, Brotschi B. Transthoracic intracardiac catheters in pediatric cardiac patients: A single-center experience. Paediatr Anaesth. 2017 Sep;27(9):918-926.
- Tannuri U, Tannuri AC, Maksoud JG. The second and third right posterior intercostal veins: an alternate route for central venous access with an implantable port in children. J Pediatr Surg. 2005 Nov;40(11):e27-30.
- Detering SM, Lassay L, Vazquez-Jimenez JF, Schnoering H. Direct right atrial insertion of a Hickman catheter in an 11-year-old girl. Interact Cardiovasc Thorac Surg. 2011 Feb;12(2):321-323.
- Birnbaum PL, Michas C, Cohen SE. Direct right atrial catheter insertion with video-assisted thoracic surgery. Ann Thorac Surg. 1996 Oct; 62(4):1197.
- Oram-Smith JC, Mullen JL, Harken AH, Fitts WT Jr. Direct right atrial catheterization for total parenteral nutrition. Surgery. 1978 Mar;83(3):274-276.
- Flori HR, Johnson LD, Hanley FL, Fineman JR. Transthoracic intracardiac catheters in pediatric patients recovering from congenital heart defect surgery: associated complications and outcomes. Crit Care Med. 2000;28(8):2997-3001.
- Pratap H, Millar J, Butt W, d’Udekem Y. Complications of intrathoracic lines placed during cardiac surgery. J Thorac Cardiovasc Surg. 2015; 149(4):1212-1213.
- Kumar TKS, Subramanian S, Tansey JB, et al. Optimum position of transthoracic intracardiac line following cardiac surgery. Interact Cardiovasc Thorac Surg..2017; 25(6):883-886.
References
Citation
L N, DJ A, S W, AJ T, RB T.Endovascular Retrieval of Transthoracic Right Atrial Catheter Fragment. Appl Radiol. 2022; (2):42-43.
March 4, 2022