Dysembryoplastic neuroepithelial tumor
Images
CASE SUMMARY
A 4-year-old female without significant medical history presented for evaluation of possible seizures. The patient’s mother stated her daughter had a 5- to 6-week history of strange, increasingly frequent movements. Each event lasted for 15-90 seconds and was associated with head slumping, hand clenching, arm stiffening, and unusual repetitive movements, such as turning in circles, repeating short phrases, or grasping at imaginary objects. The spells varied, occurring during the night or day. When each episode concluded, the child became angry, fearful, or affectionate.
IMAGING FINDINGS
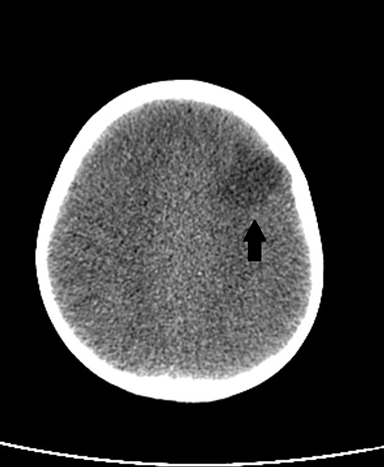
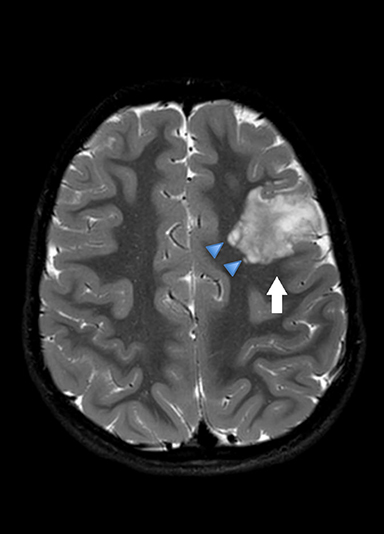
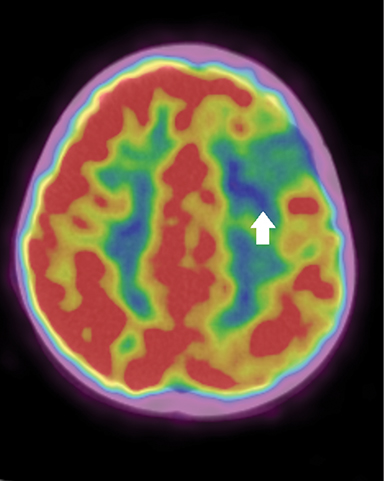
An axial noncontrast CT scan (Figure 1) revealed wedge-shaped hypodense lesion in the left frontal lobe (Figure 1), while an axial T2-weighted image (Figure 2) demonstrated a heterogeneous, T2 hyperintense lesion involving the left frontal cortex and extending into the subjacent white matter. There were areas of peripheral cystic appearance. No significant mass effect or adjacent edema was identified. Finally, axial fused PET/CT images demonstrated hypometabolism within the left frontal lobe lesion.
DIAGNOSIS
Dysembryoplastic neuroepithelial tumor (DNET). Differential diagnostic considerations included cortical dysplasia, ganglioglioma, or other low-grade neoplasm.
DISCUSSION
Dysembryoplastic neuroepithelial tumors (DNET) typically present in childhood or in young adults (mean age at onset 10 years) and can account for 20% of medically refractory epilepsy.1,2 Diagnostic criteria include partial seizure disorder that begins before age 20, no neurological deficits, and a cortically based tumor. The most common location for a DNET is the medial temporal lobe (50-80%). However, 15-25% of DNETs are found in the frontal lobe, as in this case.2 The unusual seizure manifestations in this case may have been reflected by the tumor location. Additional locations include the occipital and parietal lobes, deep cerebral nuclei (particularly caudate nuclei), cerebellum, and brainstem.
The overall appearance of DNETs varies. The tumor usually is circumscribed, wedge-shaped or cystic. On CT, DNET can demonstrate wedge-shaped cortical hypoattenuation and mimic ischemia or infection (Figure 1). The cystic (“bubbly”) appearance can help to differentiate the lesion from other tumors. The MRI appearance is T2/FLAIR hyperintensity with corresponding T1 hypointensity (Figure 2). There can be adjacent regions of cortical dysplasia. The tumor will have slow to no growth over years and can remodel the adjacent calvarium. Intratumoral calcifications may be seen in one-third of cases and peritumoral edema is exceedingly rare. The tumor can demonstrate faint nodular or patchy enhancement in 20% to 40% of cases.1 PET FDG-18 imaging will demonstrate hypometabolism within the tumor (Figure 3).
DNETs are WHO grade 1 lesions, and specific glioneuronal elements should be present on pathology that are characterized as axon columns lined by uniform oligodendroglioma-like cells with intervening floating neurons.3,4 Histology is differentiated by the subtypes, including simple (only glioneuronal elements), complex (associated with cortical dysplasia), and nonspecific (resemble low-grade glioma with no specific glioneuronal elements).3 In this case the pathology was a low-grade glioneuronal neoplasm most consistent with complex dysembryoplastic neuroepithelial tumor.
As performed in this case, gross total resection of the DNET and adjacent cortical dysplasia, if present, is the treatment of choice in DNET. Recurrence is rare, although follow-up imaging is recommended. In this case, there was no recurrence on follow-up and the patient’s symptoms improved. Tumors that recur are usually low grade; transformation into malignancy is very rare.
CONCLUSION
Dysembryoplastic neuroepithelial tumors are rare, low-grade brain tumors, with the majority presenting in individuals younger than 20 years. Imaging always plays a role in the work-up of seizures. Individuals with seizures may have normal imaging. In this case, the child’s strange behavior was secondary to the DNET. Considering an anatomic cause is important when a child presents with seizure-like symptoms. Children with a normal neurologic examination and a cortically based lesion with T2 hyperintensity and minimal mass effect should raise the possibility of a DNET.
REFERENCES
- Barkovich J, Raybaud C. Intracranial, Orbital, and Neck Masses of childhood. In: Pediatric Neuroimaging. 5th ed. Philadelphia, PA: Wolters Kluwer, Lippincott Williams and Wilkins. 2012:637-807.
- Linscott, L. DNET. Statdx Web Site. https://my.statdx.com/document/dnet/4d5ae76b-1c26-495f-881b-b66a81d21f8a?searchTerm=dnet. Updated August 2016. Accessed September 12, 2018.
- Thom M, Toma A, An S, et al. One hundred and one dysembryoplastic neuroepithelial tumors: an adult epilepsy series with immunohistochemical, molecular genetic, and clinical correlations and a review of the literature. J Neuropathol Exp Neurol. 2011; 70: 859-878.
- Abdelzaher, E. Dysembryoplastic neuroepithelial tumor (DNET). PathologyOutlines.com website. http://www.pathologyoutlines.com/topic/cnstumorDNET.html. Accessed September 12, 2018.
Citation
D M, P C, SA J, R T.Dysembryoplastic neuroepithelial tumor. Appl Radiol. 2019; (6):48-49.
November 15, 2019