Congenital myofibromatosis with pulmonary manifestations
Images


CASE SUMMARY
A 6-year-old-boy presented with hypoxia.
IMAGING FINDINGS
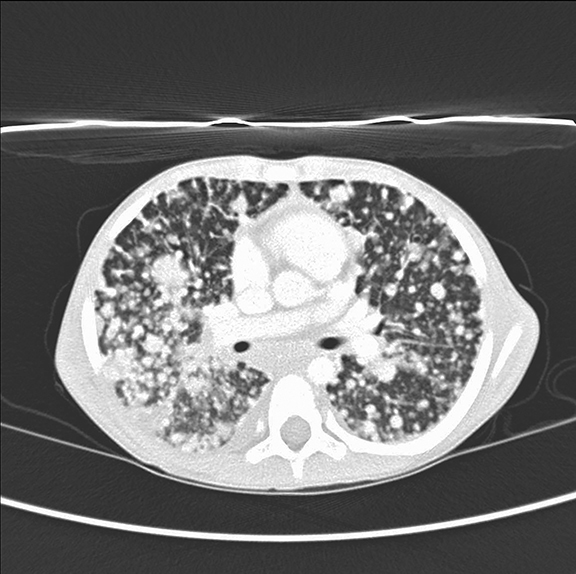
A chest radiograph (Figure 1) revealed innumerable small, non-calcified nodules throughout the chest with an approximately equal distribution between the upper and lower lobes. No osseous involvement was seen. Unenhanced axial CT image of the chest in lung windows (Figure 2) shows numerous rounded noncalcified nodules of differing sizes scattered throughout both lobes.
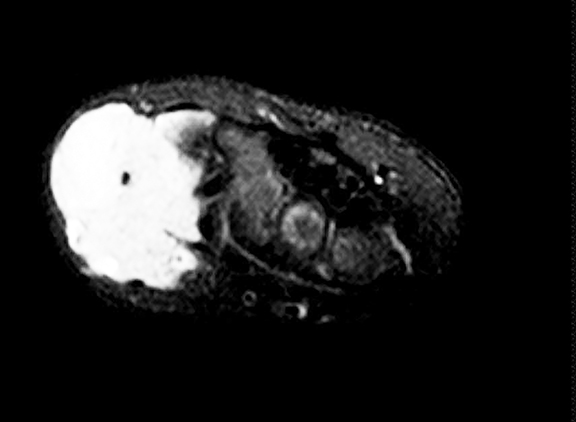
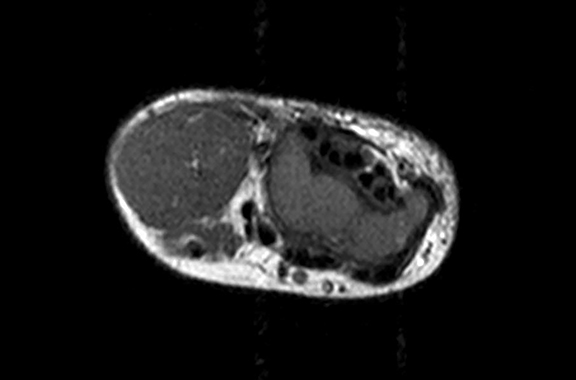
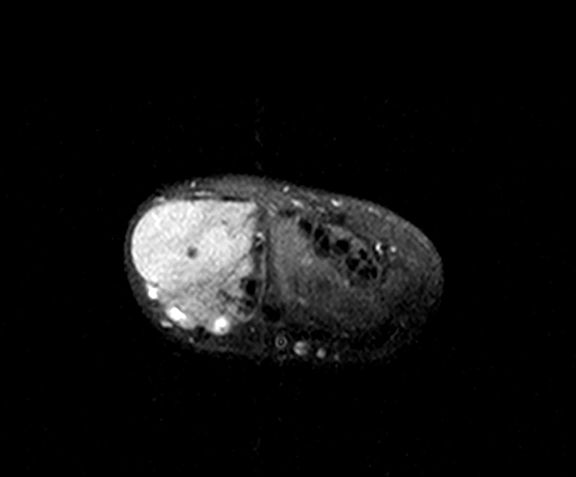
Axial MR images of the hand (Figure 3, T1, T2, T1 postcontrast) show a solid, soft tissue mass of the lateral aspect of the wrist with a homogeneous T2 bright and T1 dark appearance. The mass is homogeneously enhancing after administration of contrast. A homogeneous enhancement pattern is atypical, and a pattern of rim enhancement is most common.
DIAGNOSIS
Congenital myofibromatosis with pulmonary manifestations. The differential diagnosis includes metastatic disease, fungal/TB infection, and vasculitis.
DISCUSSION
Myofibromas are the most common fibrous tumor affecting infants. Congenital myofibromatosis (multiple lesions) typically affects children who are less than 2 years of age. Tumors can involve skin, muscle, bone, or viscera. If lesions only involve the musculoskeletal system, the prognosis is excellent. However, when viscera are involved, the prognosis is much worse. This condition is usually sporadic; however, there have been a few reports of familial involvement. Interestingly, the condition is twice as common in males compared to females.1
Clinically, a myofibroma manifests as a solitary nodule in the dermis which can measure a few millimeters to a few centimeters. If the nodule is superficial it will be mobile while it will be nearly immovable if deeper tissues are involved. The solitary type has been found to be three times more common than multiple lesions. Solitary lesions are most common in the head and neck, followed by the trunk and then the extremities. It is very rare for a solitary lesion to involve the viscera; however, solitary lesions have been found in the bones, most commonly the maxillofacial bones. In patients with multiple lesions, up to 40% may be found in the viscera. The most common sites of visceral involvement are the lungs, heart, gastrointestinal tract, pancreas, and rarely the CNS. The visceral lesions are typically present at birth. Nodules grow the most in the perinatal period but can grow later in life.
The sonographic appearance of these lesions is variable and can range from anechoic to hyperechoic with a thick wall. On CT, there is typically a peripheral rim of enhancement with the remaining lesion enhancing equal to or less than muscle. Lesions usually have bright signal on T2 imaging and low signal on T1 imaging. Radiographically osseous lesions tend to be lytic and within the metaphysis.1
Clinically, patients with lesions confined to soft tissue and bone require very little treatment, and lesions tend to regress spontaneously even if multiple. When excised, the lesions tend to locally recur. Up to 75% of patients with visceral lesions at birth die from related complications. In some cases, chemotherapy has been shown to help these patients.3
CONCLUSION
With the use of clinical, pathologic, and radiologic information congenital myofibromatosis can be diagnosed and the extent determined. The prognosis is highly dependent on the involvement of viscera which can be determined by ultrasound, CT, or MRI. In addition, accurate diagnosis should remove the need for further work up and unnecessary treatment in patients with extra-visceral disease.
REFERENCES
- Caffey J, Coley B. Caffey’s pediatric diagnostic imaging, 2013; 12th Edition. Elsevier Saunders, Philadelphia,PA
- Arcangeli F, Calista D. Congenital myofibromatosis in two siblings. Eur J Dermatol .2006;16:181-183.
- Weiss S, Goldblum J. Enzinger and Weiss’s soft tissue tumors. 2008; 5th Edition. Elsevier, Philadelphia, PA.
Citation
M P, SA J, AJ T, R T.Congenital myofibromatosis with pulmonary manifestations. Appl Radiol. 2017; (12):36-37.
December 7, 2017