Chronic Lipoid Pneumonia
Images
CASE SUMMARY
A 65-year-old with previous history of cerebral palsy, gastroparesis with severe gastroesophageal reflux, and chronic constipation, presented with acute dyspnea and desaturation.
IMAGING FINDINGS
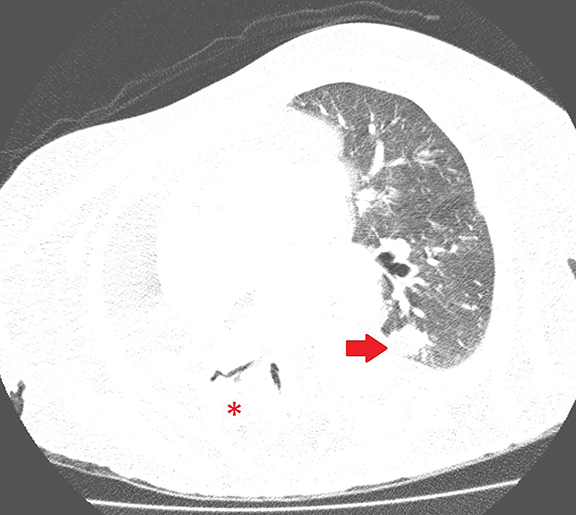
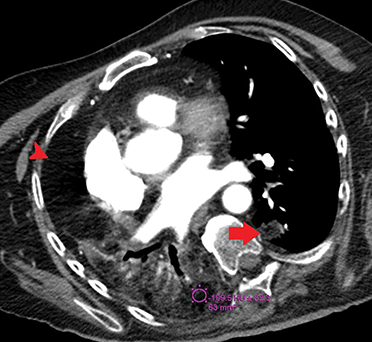
Axial chest CT in lung (Figure 1) and soft tissue (Figure 2, ) windows demonstrates airspace consolidation in the right lower lobe with areas of fat density (-109 Hounsfield Units [HU]) and nodular opacity also with fat density in the posterior segment of the left lower lobe.
DIAGNOSIS
Chronic lipoid pneumonia
DISCUSSION
Fat attenuation within lung infiltrates on CT was first described by Joshi et al in 1985.1 They reported a case of a 42-year-old with chronic cough, history of chronic mineral oil ingestion due to constipation, and extensive bilateral basal lung infiltrates with areas of fat attenuation (between -75 and -35 HU).1 Seven years later, Stern2 reported another case of consolidation with areas of fat-density and considered it diagnostic for lipoid pneumonia when associated with a history of oil ingestion.
Lipoid pneumonia was described in 1925 by Laughlin when performing autopsies on patients who were recurrently using oil-based medications. He identified the presence of oil material inside the lungs of those patients and demonstrated that tracheal oil administration in rabbits produced a similar effect. Ten years later, Graef observed that mineral oil did not irritate the pharyngeal mucosa and did not stimulate the gag reflex, facilitating its access to the lungs.3
Lipoid pneumonia can be categorized according to the lipid material involved: Primary) exogenous pneumonia (related to aspiration of animal, vegetable, or mineral oil), which can be further subdivided into acute (recent intake of lipid material) and chronic (recurrent or long-standing intake of lipid material); and Secondary) endogenous pneumonia, resulting from accumulation of endogenous lipids related to bronchial obstruction, chronic infection, alveolar proteinosis, and fat deposition diseases, such as Niemann-Pick).4,5
Exogenous lipid pneumonia may occur in patients without any risk factors; however, it usually occurs in individuals with structural abnormalities, such as cleft palate, Zenker diverticulum, tracheoesophageal fistula, hiatal hernia, and achalasia; gastroesophageal reflux disease; and psychiatric and neurological disorders, including deglutition disorders, reduced consciousness, and cognitive impairment).5
Radiographic findings of lipoid pneumonia are nonspecific; they often occur in the middle and lower lobes and include: (a) ground-glass opacities; (b) lobar, sparse, or diffuse consolidations with or without air bronchograms of peri-hilar, bibasal, segmental, or diffuse distribution; (c) reticulonodular interstitial infiltrate; or (d) poorly delimited nodules and masses.2,3,5
CT is the imaging modality of choice for the diagnosis of lipoid pneumonia. The findings of acute exogenous lipoid pneumonia usually appear between 30 minutes and 24 hours after aspiration of the lipid material. They include ground-glass opacities; bilateral, segmental, or lobar consolidation involving predominantly the middle and lower lobes; poorly delimited nodules; and other less common findings such as pneumatocele, pleural effusion, pneumothorax, and pneumomediastinum.2,4
In acute exogenous lipoid pneumonia, there may be areas of fat density within the consolidation; however, the presence of an associated inflammatory reaction may increase the density of the consolidation and mask this finding. Radiological changes are usually self-limiting, lasting 2 weeks to 8 months, while only discrete residual scar may persist.4
In chronic exogenous lipoid pneumonia, CT may demonstrate ground-glass opacities, consolidations involving one or more segments with peribronchovascular distribution affecting mainly the middle and lower lobes, nodules or masses, thickening of interlobular septa, crazy-paving opacities with basilar predominance, and other less common findings such as cavitation and calcification.2,4
The consolidations, nodules, and masses in chronic exogenous lipoid pneumonia typically present with areas of fat density (between -150 and -30 HU; the measurement should be performed away from air in the most hypodense area of consolidation.2,5
Imaging findings overlap in acute and chronic exogenous lipoid pneumonia. The only statistically significant differences described among such presentations are the presence of pleural effusion and imaging improvement on follow-up exams in acute exogenous lipoid pneumonia, and the presence of masses with fat density in chronic exogenous lipoid pneumonia.3
The differential diagnosis of these lesions includes hamartomas, lipomas, metastases of sarcomas (chondrosarcoma, liposarcoma), teratomas, and thymolipomas.5 Percutaneous, transbronchial, or open biopsy may be performed for diagnostic elucidation; however, biopsy is rarely performed in these cases. When biopsy is performed, the fragments should be frozen without being embedded in paraffin, as the process dissolves the lipids of the tissue.
Histopathological findings include lipid-laden macrophages within the alveoli and interstitium, and varying degrees of inflammatory infiltrate and fibrosis.5
CONCLUSION
Consolidation with areas of fat density is highly suggestive of chronic exogenous lipoid pneumonia, especially when associated with history of exposure to lipid material.
REFERENCES
- Joshi RR, Cholankeril JV. Computed tomography in lipoid pneumonia. J Comput Assist Tomogr. 1985; 9: 211-213.
- Stern EJ. Chronic, progressive, bibasilar infiltrates in a woman with constipation. Chest. 1992;102: 263-265.
- Baron SE, Haramati LB, Rivera VT. Radiological and clinical findings in acute and chronic exogenous lipoid pneumonia. J Thorac Imaging. 2003; 18: 217-224.
- Betancourt SL, Martinez-Jimenez S, Rossi SE, et al. Lipoid pneumonia: spectrum of clinical and radiologic manifestations. AJR Am J Roentgenol. 2010; 194:103-109.
- Marchiori E, Zanetti G, Mano CM, et al. Exogenous lipoid pneumonia: Clinical and radiological manifestations. Respir Med. 2011; 105:659-666.
Citation
A V, CP R.Chronic Lipoid Pneumonia. Appl Radiol. 2021; (3):56C-56D.
May 4, 2021