Angio-CT for Retrograde Recanalization of Chronic Celiac Artery Occlusion Prior to Radioembolization
Images





Performing angiography for Y90 “mapping” prior to radioembolization is an accepted standard protocol for treating hepatocellular carcinoma and metastatic colon cancer. In most angiography alone is sufficient to identify target regions and calculate hepatopulmonary shunt fraction, and often sufficient to account for accessory non-target vessels requiring embolization.
Catheterization of the hepatic artery may be limited in a small number of cases, however, owing to celiac artery occlusion, and prohibit sufficient catheter advancement and subsequent vessel specificity if operators are left to proceed via superior mesenteric artery (SMA) collaterals. Without such access, additional intermediate interventions such as recanalization may be needed to permit more precise and directed microsphere administration.
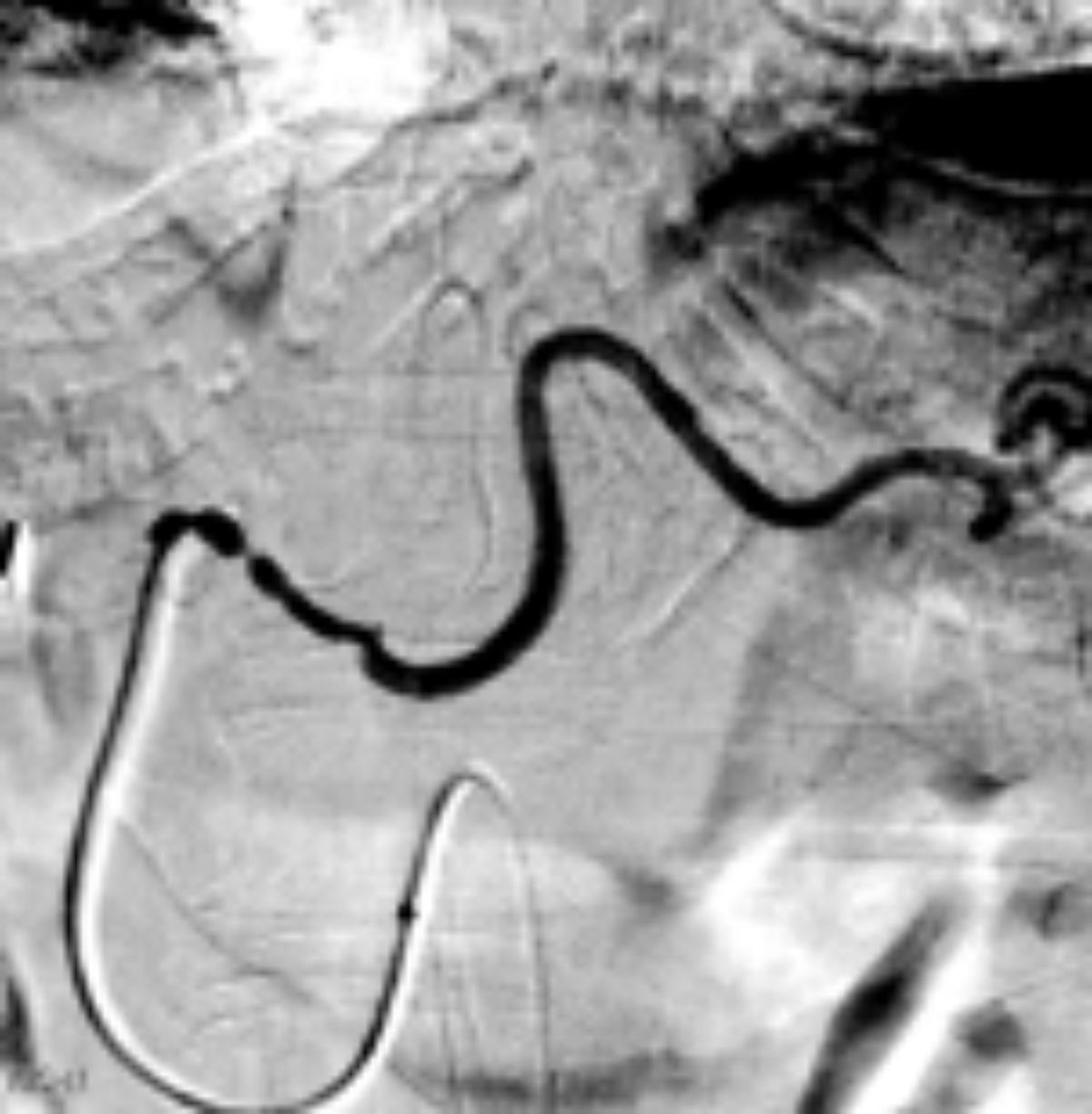
Herein we describe one example of Angio-CT being used to treat a complex flush celiac occlusion during Y90 mapping. The initial attempt to visualize the tumor, performed via the SMA through the pancreaticoduodenal arcade, was limited by vessel tortuosity, which allowed specificity beyond the hepatic lobar vessels. The Angio-CT system (4D CT, Canon Medical Systems USA, Inc.) integrates an interventional angiography system with a CT scanner on rails to permit intraprocedural CT and real-time fluoroscopy imaging.
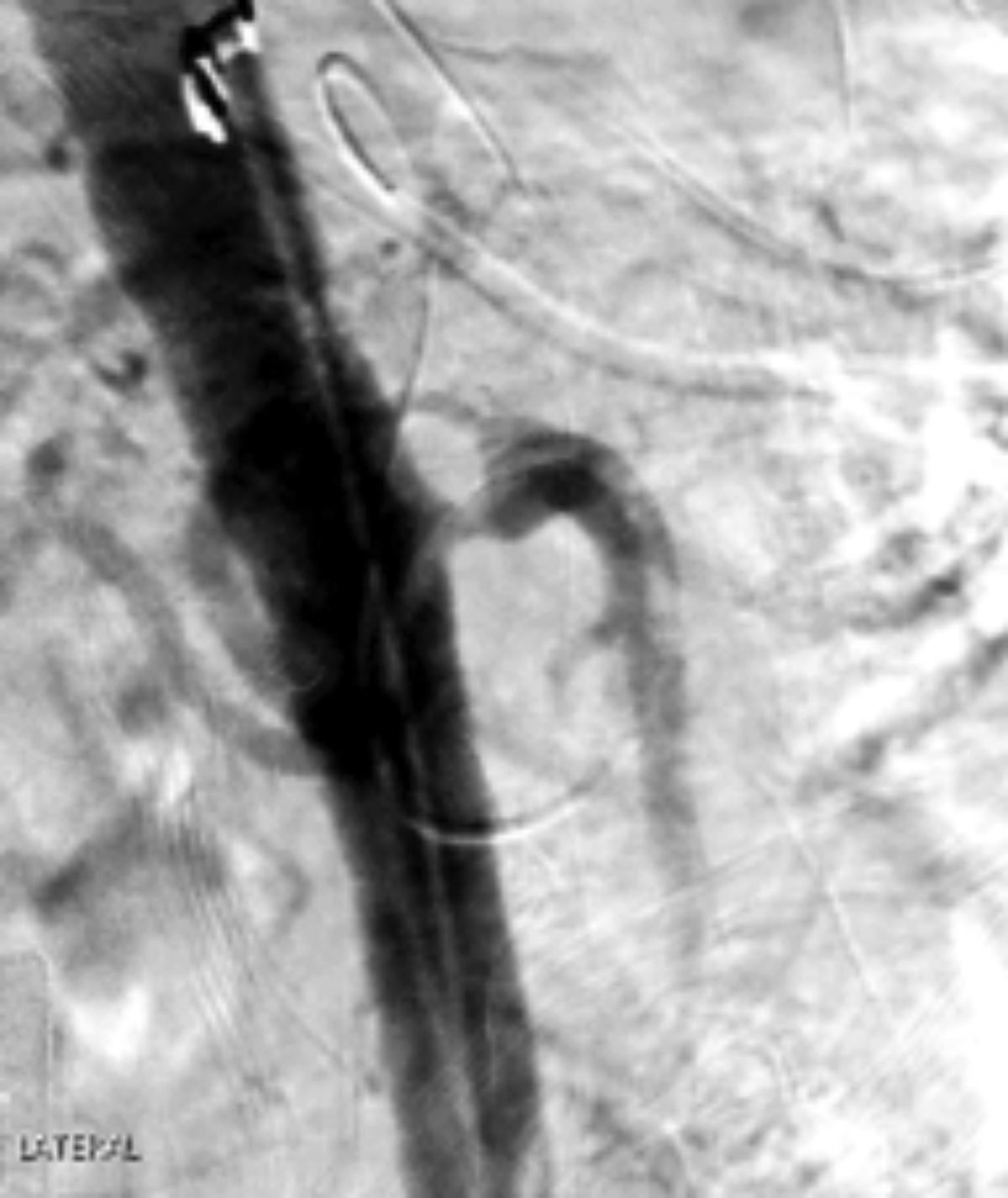
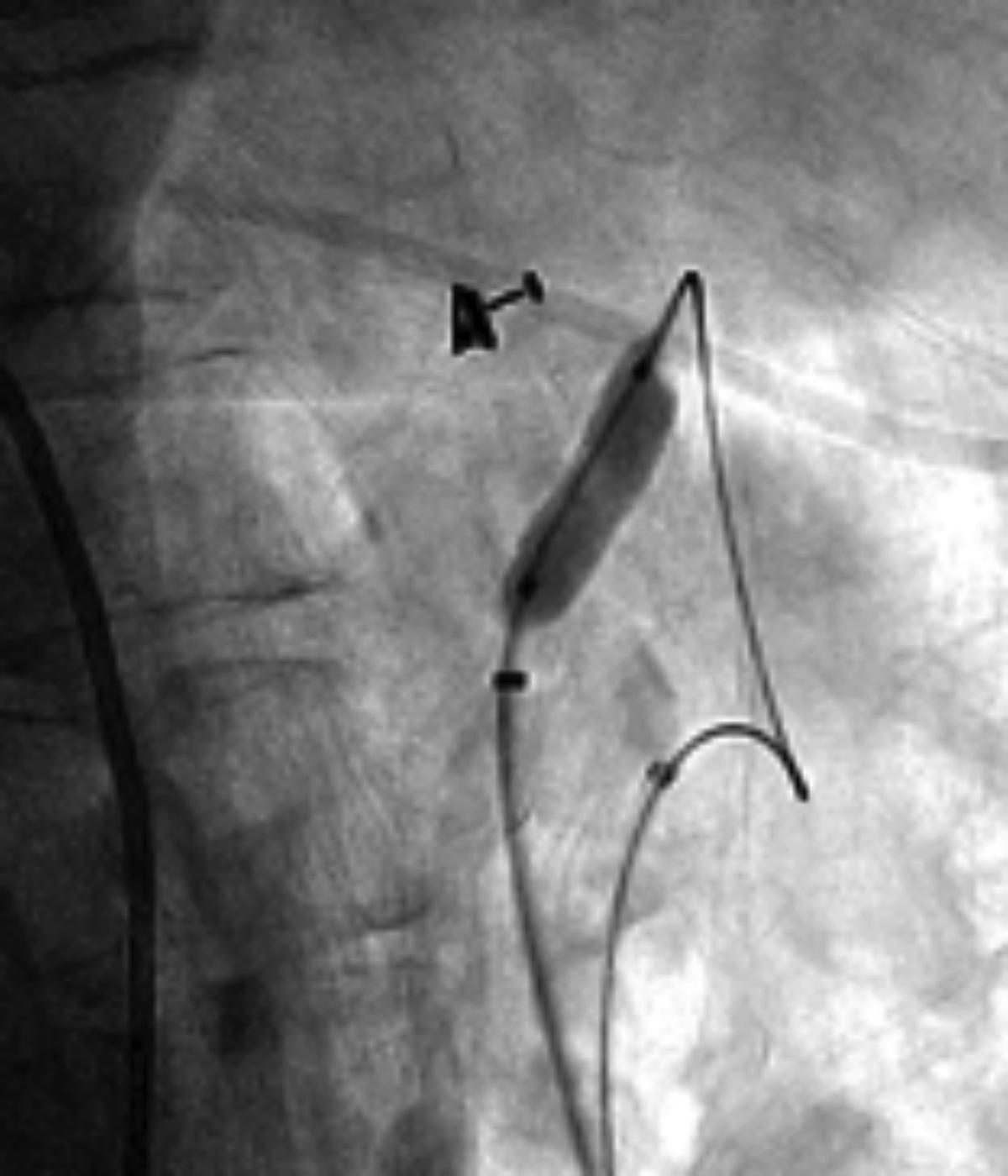
Owing to the nature of the flush occlusion and difficulty establishing its origin on lateral aortography, we were initially unsuccessful recanalizing the celiac trunk antegrade through the aorta (Figure 1). We then performed a retrograde celiac recanalization through the SMA by advancing a 4 Fr glide catheter through the gastroduodenal artery into the common hepatic artery.
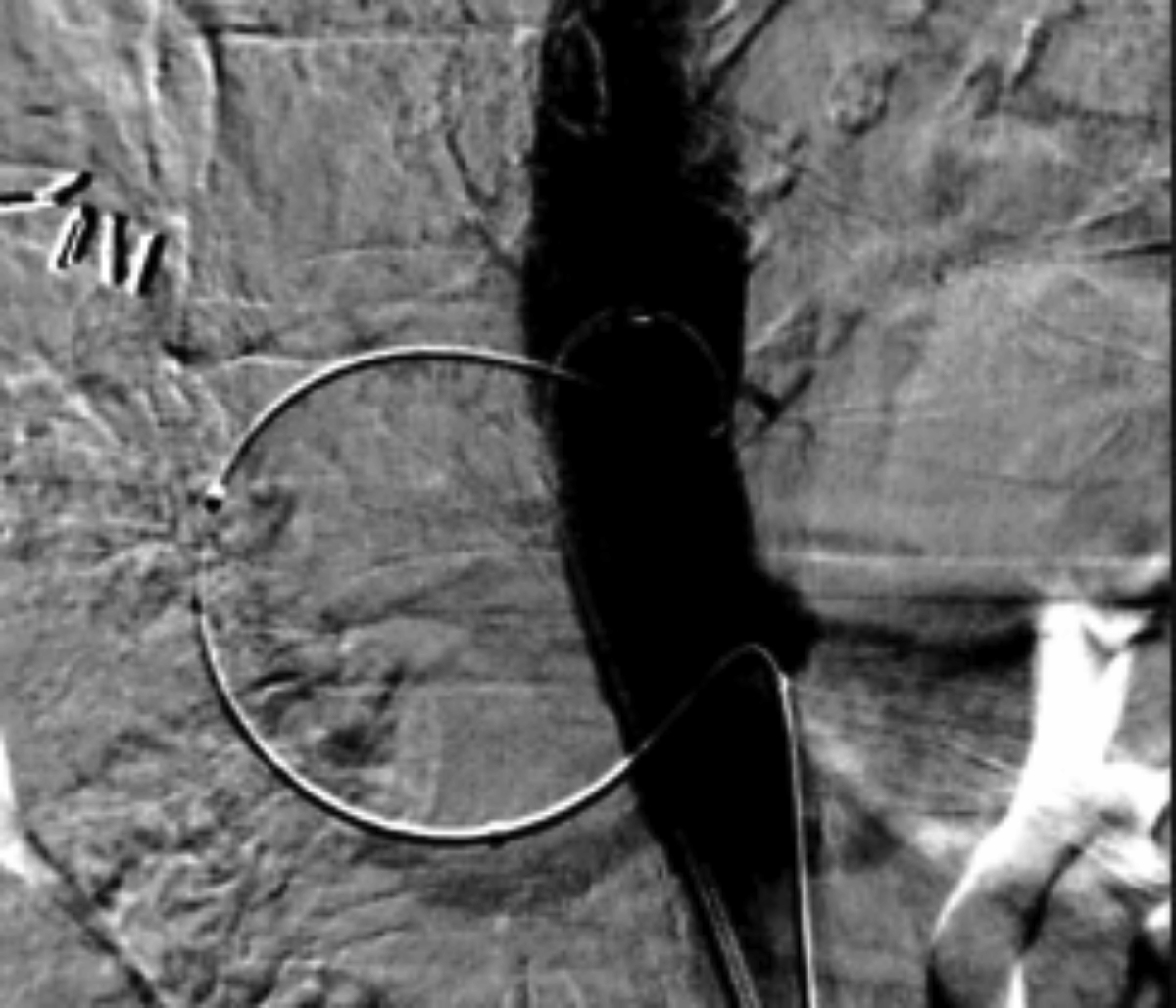
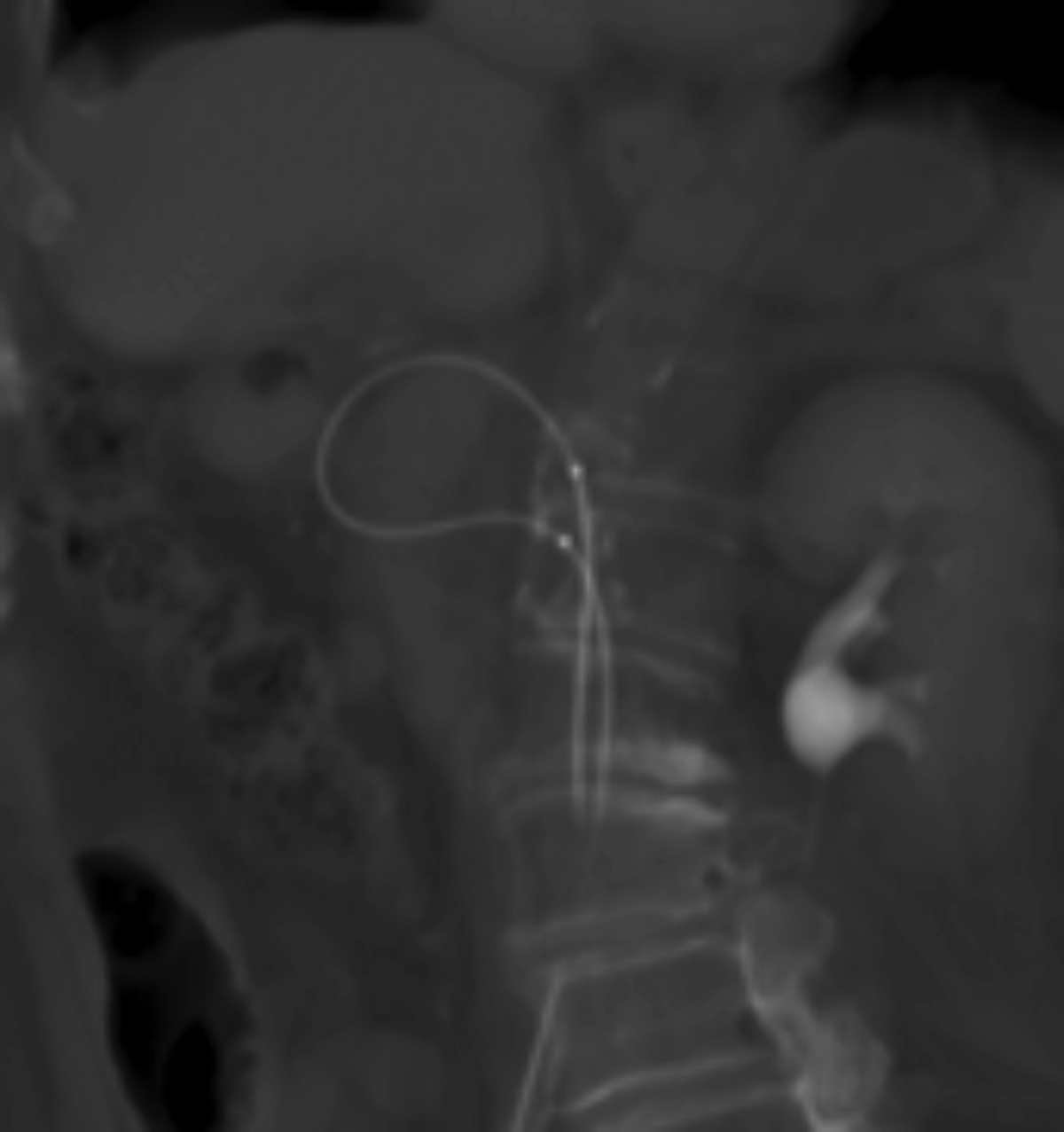
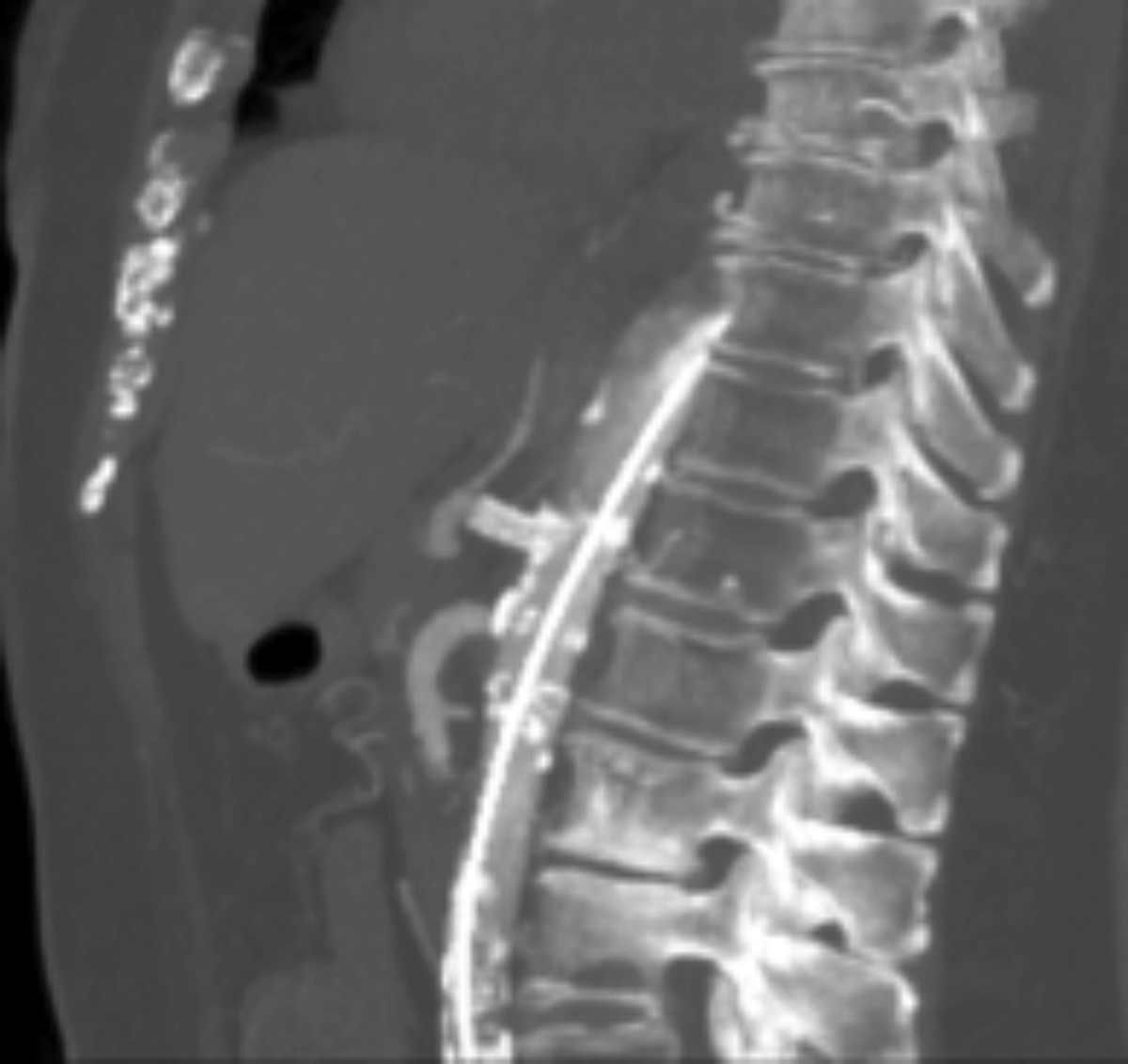
Subsequently, we used a microcatheter and double-angled glide wire to recanalize the celiac origin from a retrograde approach. This was followed by advancing a snare wire through a contralateral groin approach to establish celiac “flossing” access to facilitate stent placement. (Figure 3) Intraprocedural CT imaging acquired by the 4D CT system confirmed the optimal stent length and position before deployment in the celiac trunk. (Figure 6)
Successful recanalization and stenting allowed for sufficient contrast specificity to identify the tumor vasculature and permit Y90 segmentectomy.
In complex cases such as this example, angiography alone may not sufficiently visualize the occlusion to enable precise identification of the stent landing zone. An Angio-CT system provides adjunctive cross-sectional CT imaging that complements angiography in inconclusive cases.
In this case, the 4D CT system helped to identify stent landing zone, confirm both stent and catheter placement for targeted Y90 “mapping” and administration. This ability to analyze intraprocedural CT may provide the necessary resolution for successful and efficient recanalization, followed by angiography to precisely target placement and confirm perfusion.
This approach of using a hybrid Angio-CT system also has potential for other applications, including the identification of collateral vessels that may not be apparent using modalities such as cone-beam CT. However, such applications have yet to be assessed within a wider population.
References
- Gabr A, Ali R, Al Asadi A, et al. Technical aspects and practical approach toward same-day Y90 radioembolization in the management of hepatocellular carcinoma. Techn Vasc Intervent Radiol. 2019; 22(2): 93–99. https://doi.org/10.1053/j.tvir.2019.02.009
- Lionberg, A, Nijhawan K, Navuluri R, et al. Hybrid angiography-CT for transarterial radioembolization: a pictorial essay. Abdom Radiol. 2021:46(6): 2850–2854. https://doi.org/10.1007/s00261-020-02914-8
References
Citation
Angio-CT for Retrograde Recanalization of Chronic Celiac Artery Occlusion Prior to Radioembolization . Appl Radiol.
October 26, 2021