Acute, Transient Thyroid Swelling after Fine-needle Aspiration Biopsy
Images
Case Summary
An adult with a history of asthma and inflammatory bowel disease underwent ultrasound-guided, fine-needle aspiration (FNA) of a thyroid nodule. Three FNA passes were uneventful, but the patient reported neck pain and fullness. There were no abnormalities by ultrasound or physical exam at that time. Cytopathology requested additional sampling for diagnostic adequacy. During three additional FNA passes, an observable swelling developed in the lower neck, and ultrasound showed diffuse thyroid enlargement with a heterogeneous and edematous appearance but no hematoma. The biopsy concluded and cold compression was applied. The patient was observed for 90 minutes. The symptoms improved and there was reduction in thyroid size. At no point was there respiratory compromise. The patient reported resolution of symptoms aside from residual odynophagia at follow-up three days after the biopsy.
Imaging Findings
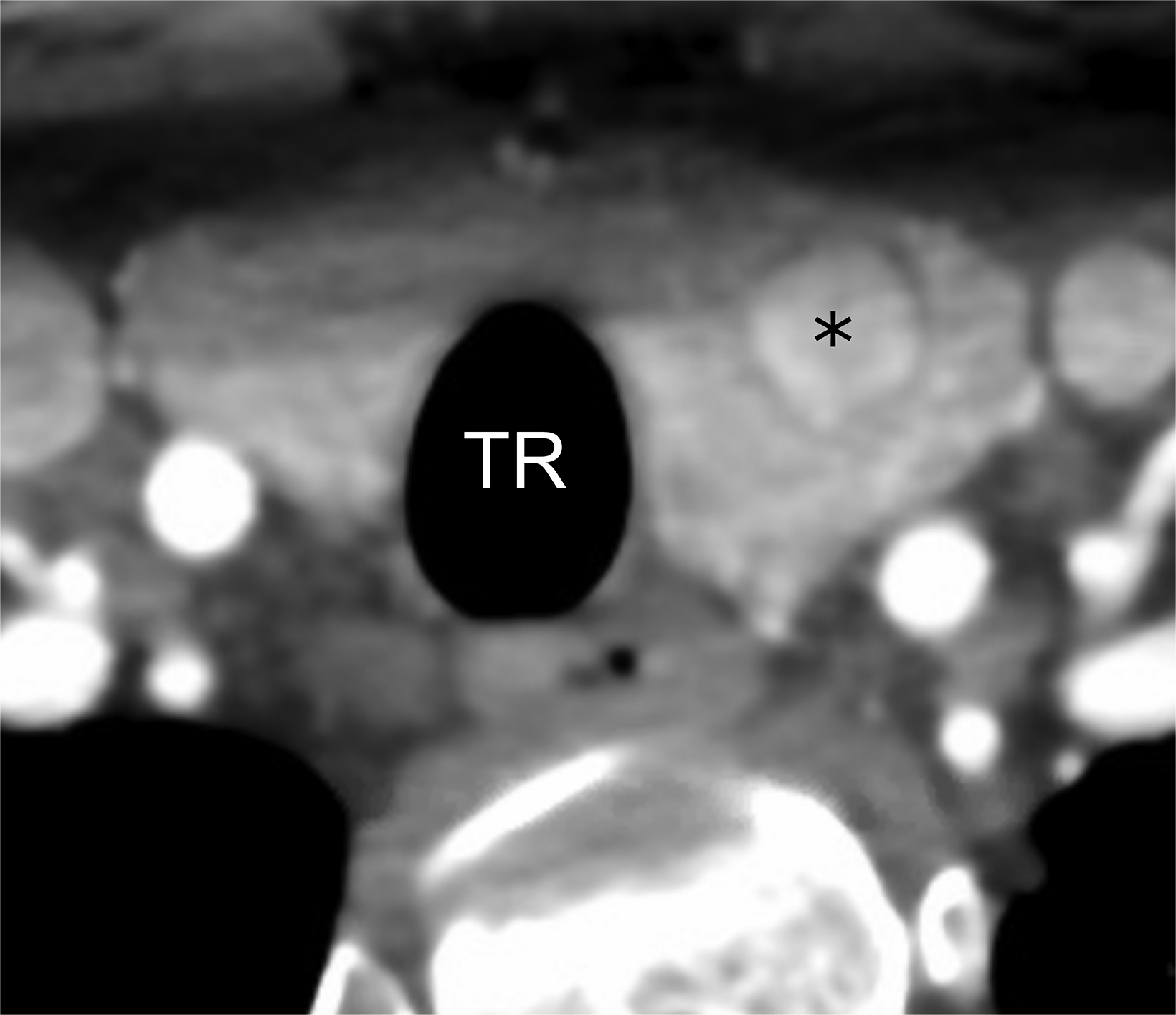
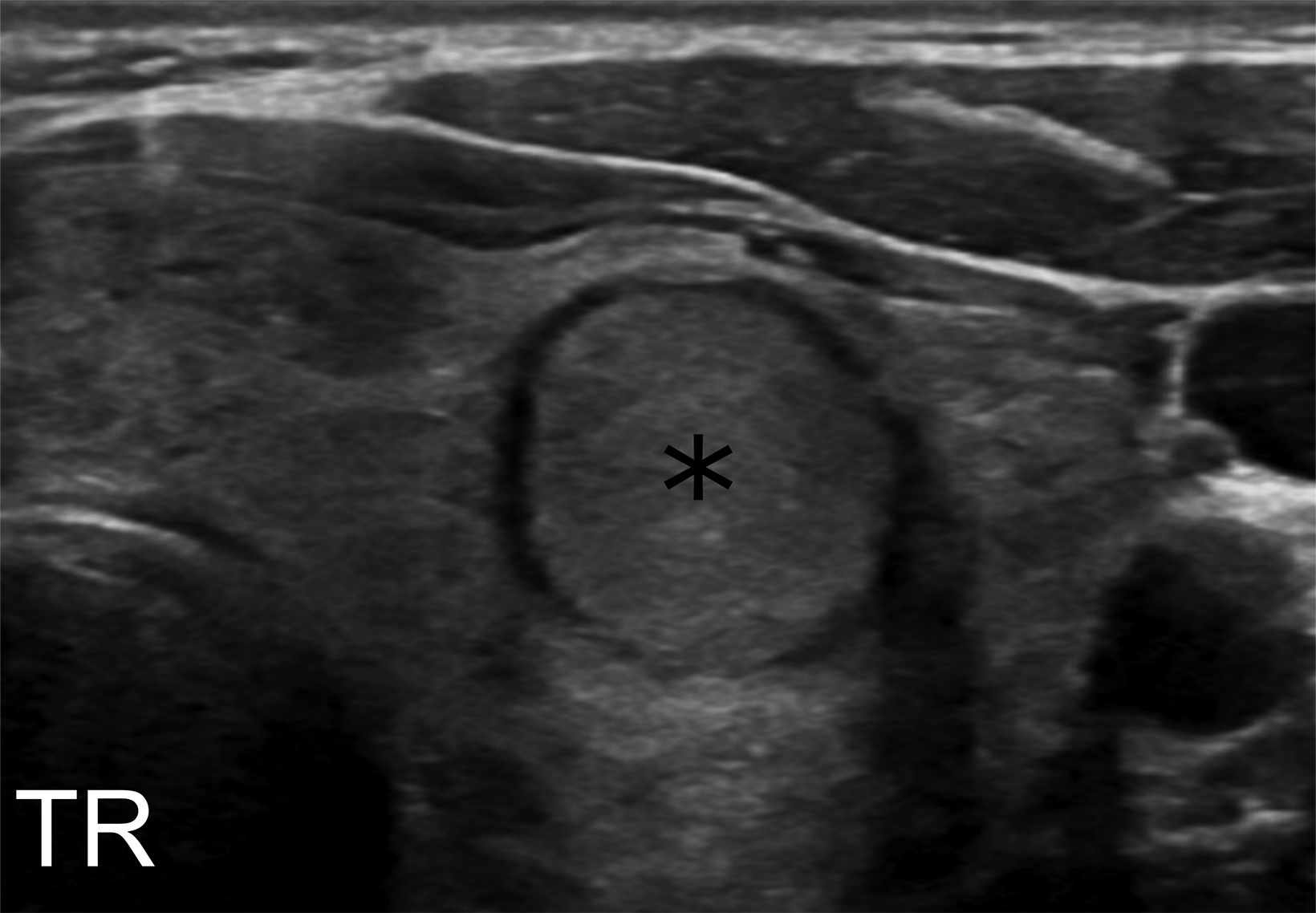
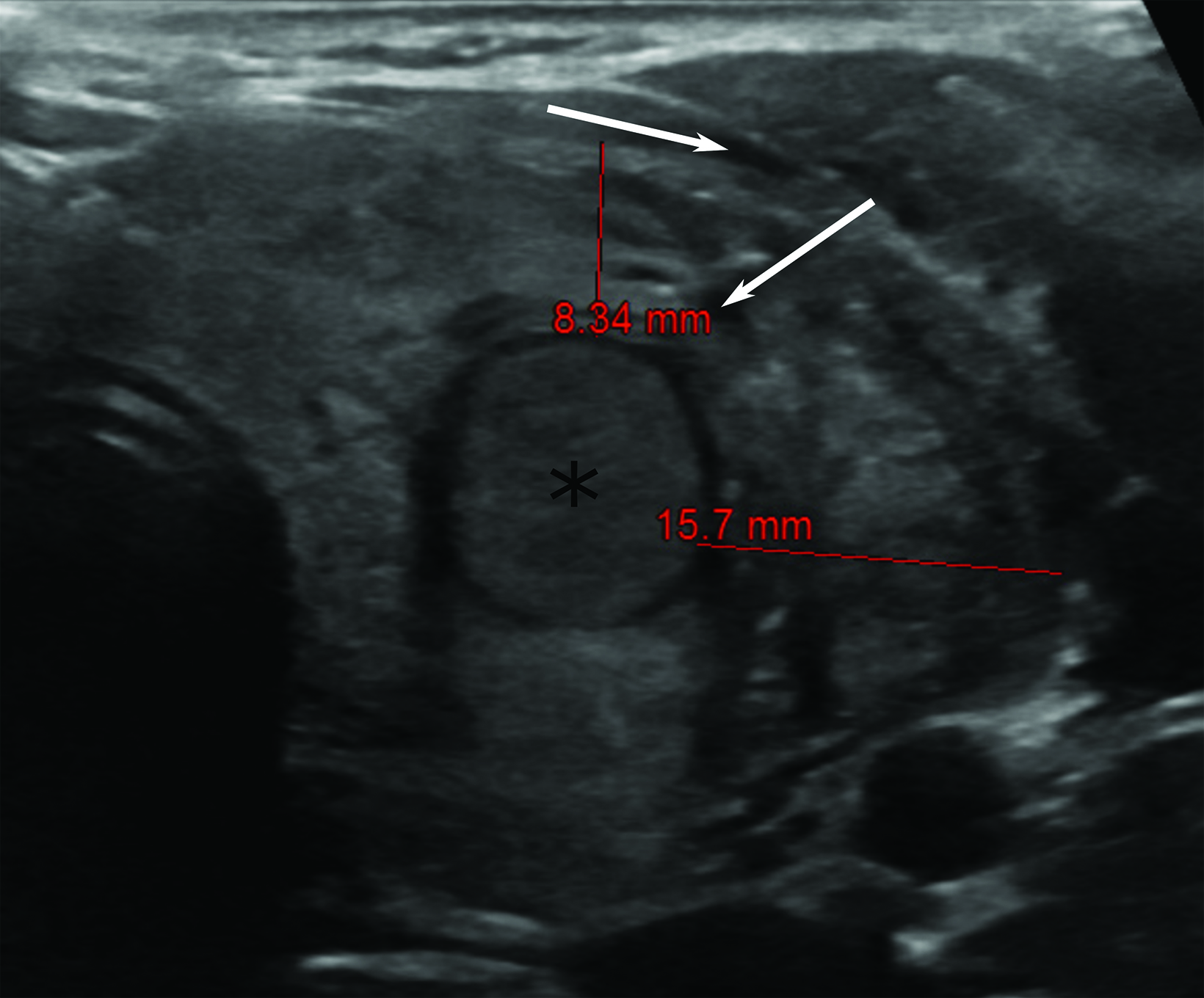
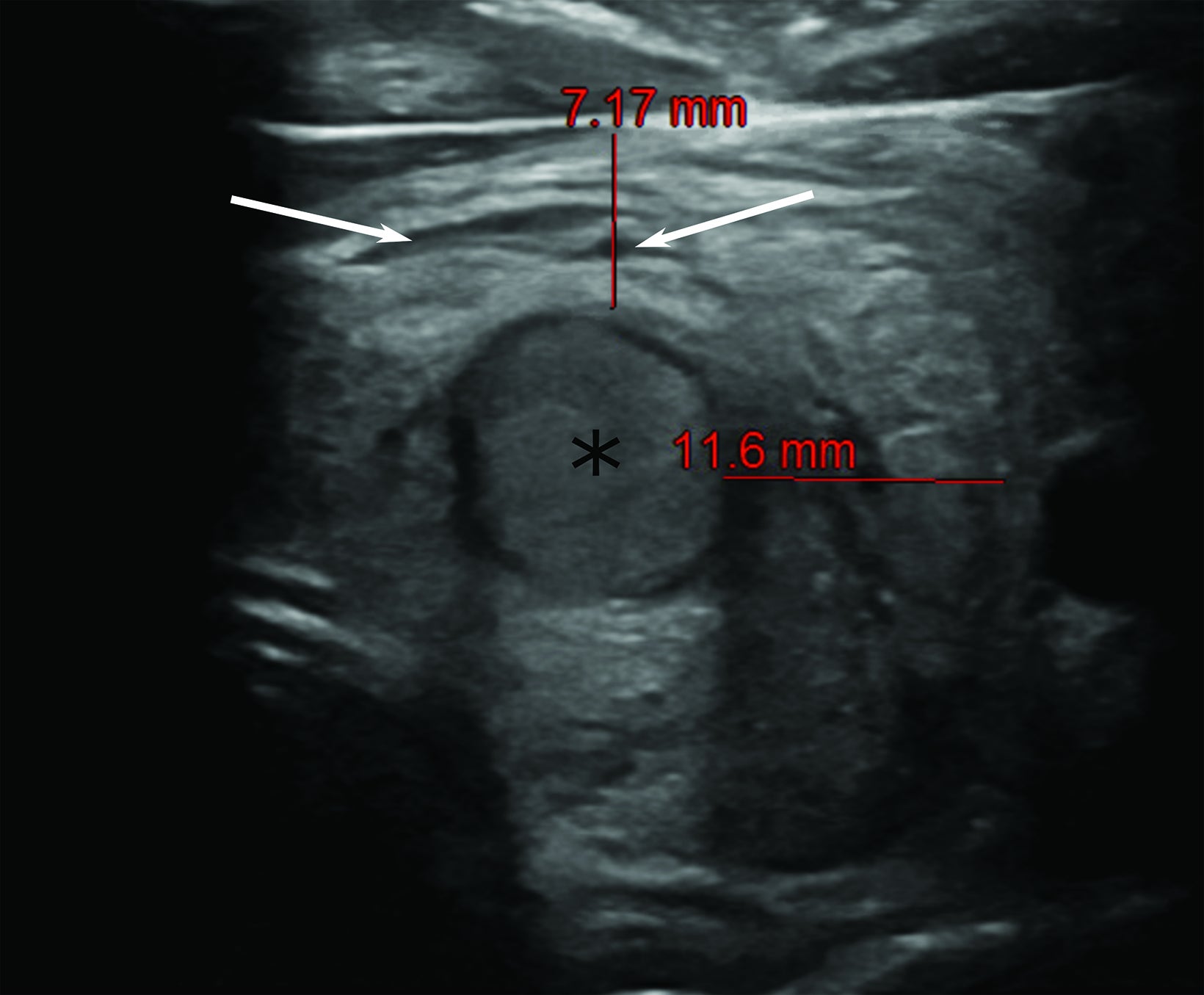
Computed tomography (CT) one month prior revealed an incidental, 1.3 cm nodule within the left thyroid lobe (Figure 1). In accordance with American College of Radiology guidelines, ultrasound imaging was performed and FNA scheduled.1 Pre-procedure ultrasonography of the left thyroid lobe confirmed presence of the nodule, which was surrounded with normal homogeneous thyroid tissue (Figure 1). Fifteen minutes after onset of symptoms, there was visible thyroid swelling and diffuse enlargement with edema and linear hypoechoic areas (cracks, Figure 2). The thyroid almost doubled in size before resolving over the two hours after onset of symptoms.
Diagnosis
Acute and transient thyroid swelling after fine-needle aspiration biopsy.
Discussion
Acute and transient thyroid swelling after FNA, sometimes referred to as cracking thyroid, is a rare and poorly understood complication of thyroid biopsy. Cracking thyroid is estimated to occur in approximately 0.1% of FNA biopsies, although the incidence is considerably uncertain given its rarity and potential under-reporting of cases.2
Despite its name, acute thyroid swelling after FNA does not appear to be limited to these procedures. A retrospective study of core-needle biopsies found that thyroid edema without hematoma occurred at a similar rate of 0.09% of thyroid nodules sampled.3 Unfortunately, the authors did not report on the ultrasonographic appearance of the thyroid following core-needle biopsy. However, given the rapid resolution of symptoms, the same etiology was likely in both procedures. Curiously, this phenomenon and imaging appearance has also been observed after subclavian vein catheterization (although the thyroid may have been inadvertently disturbed during the procedure) and during administration of recombinant tissue plasminogen activator.4,5
The pathophysiology underlying acute and transient thyroid swelling is poorly understood. In all cases, resolution is rapid and hematoma is absent, suggesting profound vasodilation or vascular leakage rather than bleeding as the source of swelling. Mechanisms proposed to account for the vasodilation implicate the release of vasoactive substances such as calcitonin gene-related peptide or histamine from mast cell degranulation.6,2
Our patient had a history of atopic disease, including known asthma and inflammatory bowel disease. There is some suggestion that atopic conditions may predispose patients to this type of rare procedural reaction, given the role of histamine in the pathophysiology of atopy and the strong correlation of atopy with other allergy-like reactions.7,8 Regardless, there is no clear relationship between patient age, gender, medical history, or underlying thyroid pathology and development of acute and transient thyroid swelling.
Rapid and profound thyroid enlargement is alarming and potentially dangerous given its proximity to the trachea. Fortunately, the condition generally appears to be benign and largely self-limited, resolving spontaneously in a matter of hours. Close observation and conservative management with cold compression is likely sufficient, although others have given diclofenac or acetaminophen.9 Corticosteroids have also been administered, but as swelling typically resolves before the expected onset of steroid activity, their value is unclear.1,10
Improved awareness of this rare and benign complication will help reduce the risk of unnecessary and potentially harmful interventions such as administration of epinephrine or referral to an emergency department, while additional case reports may provide insights into the causative mechanisms.
Conclusion
Acute and transient thyroid swelling after FNA biopsy is a rare complication that presents with thyroid swelling, anterior neck pain, and appearance of hypoechoic linear areas (cracks) in the thyroid on ultrasound. While its pathophysiology is unclear, the condition occurs in 0.1% of thyroid biopsies and appears to be benign and self-limited, with signs and symptoms resolving within an hour or two. The condition can be managed successfully with close observation and cold compression. As acute and transient thyroid swelling can be alarming to both the patient and proceduralist, awareness of this complication can prevent unnecessary interventions and lead to more appropriate patient care.
References
- Tessler FN, Middleton WD, Grant EG, et al. ACR thyroid imaging, reporting and data system (TI-RADS): white paper of the ACR TI-RADS committee. J Am Coll Radiol. 2017; 14:587-595.
- Mizokami T, Hamada K, Maruta T, Higashi K, Tajiri J. Acute and transient thyroid swelling following fine-needle aspiration biopsy: its prevalence, clinical features, and ultrasonographic findings. AACE Clinical Case Reports. 2018; 4:e134-e139.
- Ha JE, Baek JH, Lee JH, et al. Complications following US-guided core-needle biopsy for thyroid lesions: a retrospective study of 6,169 consecutive patients with 6,687 thyroid nodules. Eur Radiol. 2017; 27:1186-1194.
- Bouwman RA, Meijerink MR, Beishuizen A. Acute transient thyroid swelling after catheterization of the subclavian vein. Critical Care. 2009; 13(5):419-420.
- Shi L, Yan C, Xu W, Huang P. Acute diffuse and transient thyroid swelling after intravenous thrombolysis for acute ischemic stroke. Medicine. 2018; 97:36-38.
- Van den Bruel A, Roelandt P, Drijkoningen M, Hudders J-P, Decallonne B, Bouillon R. A thyroid thriller: acute transient and symmetric goiter after fine-needle aspiration of a solitary thyroid nodule. Thyroid. 2008; 18(1):81-84.
- White MV. The role of histamine in allergic diseases. J Allergy Clin Immunol. 1990; 86(4 Pt 2):599-605.
- Pinart M, Benet M, Annesi-Maesano I, et al. Comorbidity of eczema, rhinitis, and asthma in IgE-sensitised and non-IgE-sensitised children in MeDALL: a population-based cohort study. Lancet Respir Med. 2014; 2:131-140.
- Norrenberg S, Rorive S, Laskar P, et al. Acute transient thyroid swelling after fine-needle aspiration biopsy: a rare complication of unknown origin. Clin Endocrinol. 2011; 75:568-570.
- Gibson PG, Saltos N, Fakes K. Acute anti-inflammatory effects of inhaled budesonide in asthma. Am J Respir Crit Care Med. 2001;163:32-36
References
Citation
AF V, AD K, LM G.Acute, Transient Thyroid Swelling after Fine-needle Aspiration Biopsy. Appl Radiol. 2022; (3):44-46.
April 26, 2022