Acetabular fractures: A Stepwise approach to identification and classification on 2D computed tomography
Images














Acetabular fractures result from either high-energy trauma such as motor vehicle accidents, or low-energy trauma such as falls, especially in the elderly. Data from meta-analysis has reported that 80.5% of acetabular fractures result from motor vehicle accidents and 10.7% result from falls.1-4
The fracture classification system developed by Judet and Letournel is the most widely accepted system; it differentiates fractures into ten types, five elementary fractures and five associated fractures based on observations from plain radiographs.5-7 Adequate treatment of acetabular fractures requires an accurate definition of the type of fracture, the degree of comminution, and the presence of intraarticular debris.8 Classifying acetabular fractures is challenging, yet vitally important to selecting the best surgical strategy and approach.9,10
In this article, we provide a step-by-step diagnostic method that relies exclusively on axial CT images to avoid confusion while evaluating different fracture types and to improve the accuracy of diagnosing the fracture pattern without relying on 3D images. The decision trees obtained from this approach are well suited to everyday practice. Since 3D reconstructions are widely used in preoperative planning and classification, however, we recommend performing the reconstructions and providing them for surgeons, as these images tend to demonstrate concomitant abnormalities such as intra-articular fracture fragments, impactions, and degree of comminution. Moreover, 3D reconstructions are increasingly being used in preprocedural plate fabrication, “virtual reductions,” and intraoperative augmented reality.
Acetabular fractures: Standard procedure
Fractures of the acetabulum are usually diagnosed by conventional radiography, axial CT, and three-dimensional CT (3D CT).11 Whole-body MDCT is the most commonly performed technique evaluating patients with polytrauma.12 The high-quality thin-section axial CT data obtained during initial scanning can be used to perform coronal and sagittal multiplanar reconstructed (MPR) images, and surface-rendered three-dimensional (3D) reconstructions.
The complex anatomy of the acetabulum makes accurate depiction of the fracture type and the true extent of the fracture difficult by conventional radiographs and axial CT images. However, axial CT is extremely sensitive in detecting fractures, especially subtle nondisplaced fractures.11,13 For fracture pattern identification on axial CT images, the complex three-dimensional anatomy of the acetabulum requires a thorough mental integration of multiple axial images to provide an accurate classification of the complex fracture patterns.14 Nevertheless, diagnostic errors remain common, particularly among inexperienced surgeons and radiologists due to the complicated nature of acetabular fractures that traverse the complex anatomy of acetabulum in various directions.15
Advances in data processing allow for rapid generation of reformatted 3D images of the acetabulum that aids in accurately characterizing complex acetabular fractures.11 Fractures are described relative to their orientation to the acetabulum as viewed en face from the lateral side. Such en face 3D acetabular anatomy can be demonstrated by subtracting the femoral head from the acetabulum. These reconstructions, performed at a separate workstation, have demonstrated improvement in diagnostic accuracy and reproducibility of acetabular fractures, compared to axial CT images when used by orthopedic surgeons, but have failed to show significant improvement for radiologists.16 In addition, 3D reconstructions require considerable time, especially if the femoral head must be subtracted from the acetabulum. This time factor is the main limitation of 3D reconstruction in busy trauma or emergency departments, despite its ability to more accurately classify fractures. As long as thin-section axial images are acquired, 3D volume rendered images can be obtained later if necessary to help surgical planning.
Normal Anatomy
Columns and walls
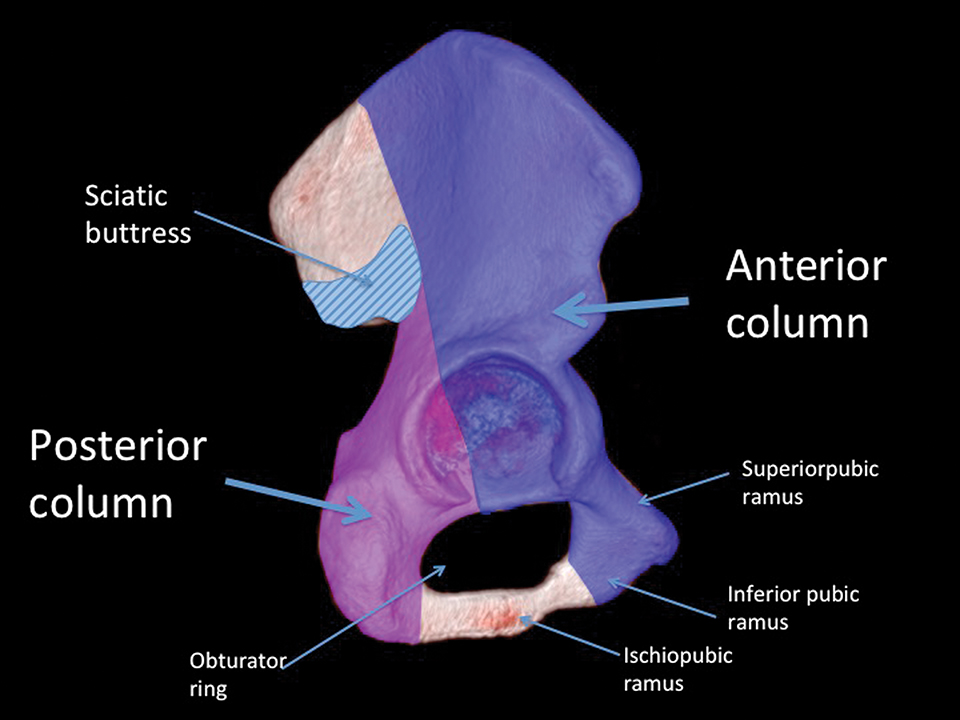
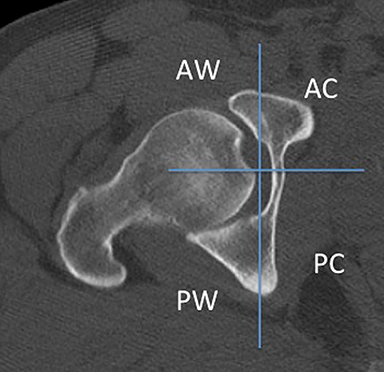
The acetabulum is formed by a large anterior and a smaller posterior column (Figure 1). The former comprises the superior pubic ramus, anterior half of the acetabulum (viewed en face), and the anterior two-thirds of the iliac wing, extending to the iliac crest. The posterior column comprises the ischial tuberosity and posterior half of the acetabulum, and it ends at the level of the greater sciatic notch. The two columns join in the supra acetabular region.17-19 The anterior and posterior walls extend laterally from the respective columns and stabilize the hip joint in the anterior and posterior directions (Figure 2). In contrast to the anterior wall, the posterior wall is larger and more frequently fractured.
Sciatic buttress
The sciatic buttress is a rectangular strut of ilium connecting the anterior and posterior columns to the axial skeleton through the sacroiliac joint (Figure 1). It is positioned above the greater sciatic notch at the superior confluence of the columns.
Obturator ring
The obturator ring is formed by the superior and inferior pubic rami and the ischial ramus (Figure 1).
Quadrilateral plate
The quadrilateral plate or surface is the relatively smooth medial surface of the pelvis at the confluence of the innominate bones deep to the obturator internus muscle; it is a significant portion of the posterior column. Fractures involving the medial acetabular wall will disrupt the plate.
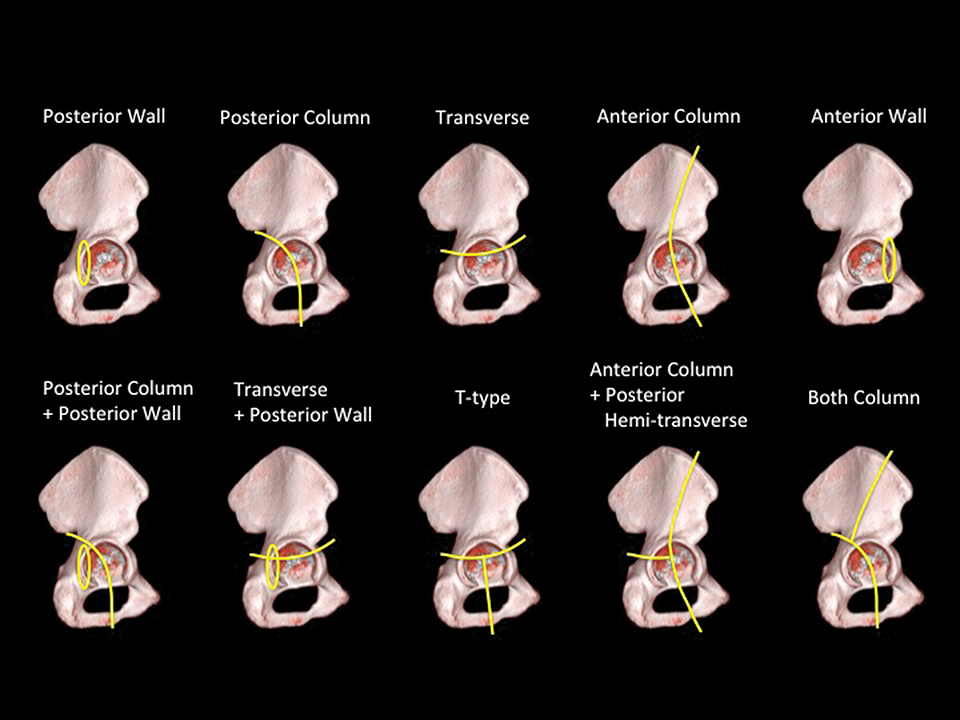
Fracture classification
Acetabular fractures comprise 10 different types: five elementary fractures and five associated fractures as described by Judet and Letournel (Figure 3).5 Four of the elementary fractures are named for the anatomy of the acetabulum: anterior wall, posterior wall, anterior column, and posterior column fractures. The fifth elementary fracture pattern is the transverse fracture, which bisects the anterior and posterior columns and divides the acetabulum into upper iliac and lower ischiopubic segments. It may be easier for fracture classification, however, to organize all ten fracture types by column-type fractures, transverse-type fractures, or wall-type fractures.
Six steps to evaluating acetabular fractures on 2D CT
A systematic approach to axial CT images with a standardized checklist of sequential questions provides enough information to classify most acetabular fractures. Our approach starts with a search for fracture lines and then proceeds to an initial classification of the fracture into one of three main groups: column-type fractures, transverse-type fractures, and wall-type fractures. The fracture is then further classified to one of the 10 types based on imaging features.6,7,20 Complicated cases with severe comminution may not fit neatly into any one type; in these cases, the fracture should be classified according to the closest matching type, with appropriate qualifications. These types of atypical fractures are not uncommon.
We begin by scrolling through the acetabulum to confirm the presence of a fracture. Upon confirmation, we then scroll down to evaluate the obturator ring for disruption, then up to the articular surface to determine fracture line orientation, paying specific attention to the acetabular roof, the base of the walls, and the quadrilateral plate to classify them into one of the three main groups.
Step 1. Interrogate axial images at the acetabular articular level to confirm the articular surface of acetabulum involved to begin the approach. Determine the presence, if any, of isolated wall fractures. Isolated simple wall fractures disrupt the lips of the acetabulum without breaking either column or any other acetabular component (Figure 4). Column fractures and transverse fractures, on the other hand, involve the quadrilateral surface, the flat medial surface of the acetabulum (Figure 5). The wall fracture lines usually have an oblique orientation on CT scans without involving the quadrilateral surface (Figure 4). Posterior-wall fractures should be examined more carefully for degree of comminution, dominant fragment size, and extension into the roof or superior rim of the acetabulum, all of which have implications for surgical management.
Step 2. In patients with quadrilateral surface involvement, scroll down to determine if the fracture extends through either the inferior pubic ramus or the ischial tuberosity to establish involvement, if any, of the obturator ring (Figure 5A, 6 [level 1]). In rare instances, fractures of the superior pubic ramus can indicate obturator ring disruption. Obturator ring involvement narrows the differential to column or T-type fractures (Figure 6).
Step 3. Scroll up and interrogate the images at the articular surface to determine fracture-line orientation through the quadrilateral surface and differentiate column fractures from transverse fractures (Figure 6). In column fractures, the dominant fracture extends through the quadrilateral plate from lateral to medial in a close approximation to the anatomic coronal plane (Figure 5). Conceptually, in a column pattern, the acetabulum is disrupted with a more or less vertical fracture line and broken into front and back pieces (Figure 5E).19,21 This is opposed to the transverse fracture, defined by a dominant fracture line traversing the anterior and posterior column in a close approximation to the anatomic sagittal plane (Figure 7). It is worth noting that the classic description of acetabular fractures is from the surgeon’s perspective, not the radiologist’s. As such, a “transverse” fracture plane when the acetabulum is viewed en face with the acetabular notch oriented inferiorly becomes a near-sagittal fracture plane on axial images with the acetabulum in anatomic position (Figure 7). A transverse fracture involving the obturator ring makes the fracture a T-type fracture (Figure 6). With the T-shaped fracture, the superior fragment above the fracture line is similar to an elementary transverse fracture.
Step 4. This step consists of evaluating for fracture extension into the iliac wing above the acetabulum (Figure 5). Iliac wing fractures are detected easily and reliably from slices above the dome of the acetabulum (Figure 6). An iliac wing fracture is pathognomonic of anterior column fracture. But, if, instead of extending into the iliac wing as seen with anterior column fracture, the column fracture extends to the greater sciatic notch, it is diagnostic of a posterior column fracture (Figures 6, 8).
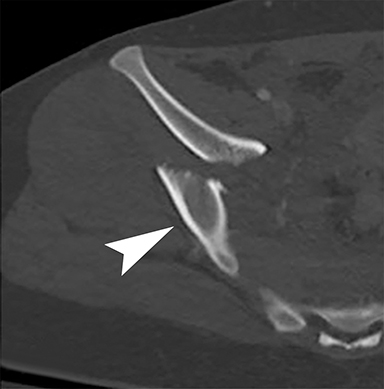
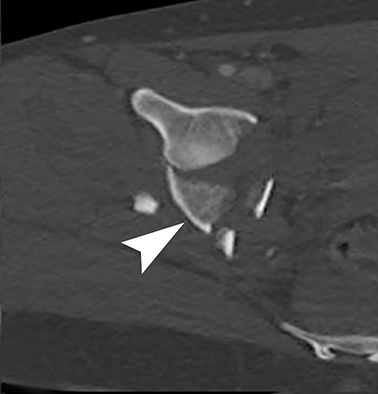
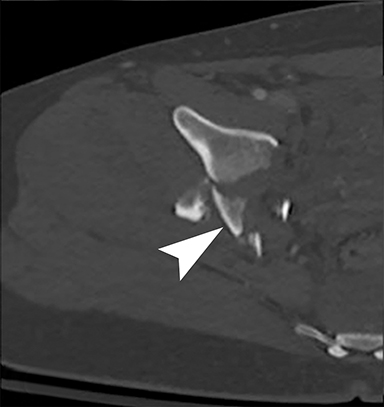
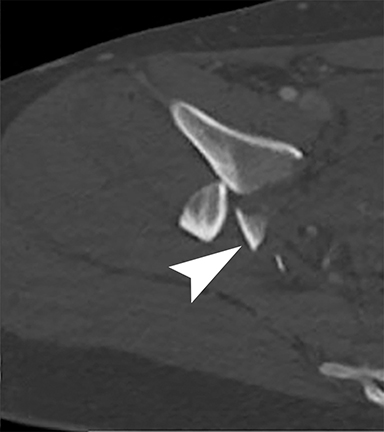
Step 5. This step consists of differentiating the associated fractures with anterior column fracture. The two associated fractures with anterior column involvement are the dual-column fracture and the anterior column-with-posterior hemitransverse fracture. Image review should begin at the inferior aspect of the sacroiliac joint and identifying the sciatic buttress. Scroll down, following the sciatic buttress caudally through the posterior column into the acetabular roof. If there is lack of continuity between the sciatic buttress and posterior column prior to reaching the acetabular joint surface, or if the buttress is not contiguous with any of the articular surfaces, both columns are fractured (Figure 9).
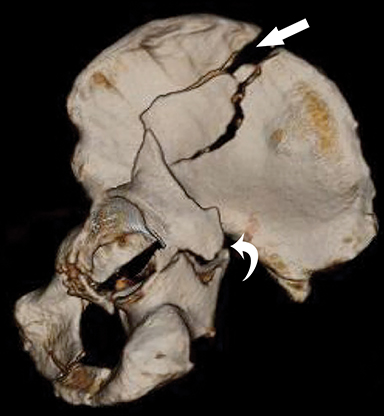
If present, the sciatic buttress will taper to a triangular extension of bone, projecting inferiorly and laterally from the sacroiliac joint and discontinuous from the articular surface — the so-called “spur sign.” (Figure 9) When both columns fracture, no support exists between the weight- bearing acetabular articular surface and the axial skeleton through the sacroiliac joint. However, a sciatic buttress that continues uninterrupted through the posterior column to terminate within the joint surface of the acetabulum is diagnostic of an anterior column-with- posterior-hemitransverse fracture (Figure 10).
Step 6. This final step focuses on two of the associated posterior wall fractures. These are the posterior column-with-posterior wall, and transverse-with-posterior wall fractures (Figures 7, 8). We have already shown how to identify isolated posterior column and isolated transverse fractures. The associated fractures are present when the isolated fractures include posterior wall detachment and can be identified separately as a free fragment (Figures 7, 8). Note that a transverse-type fracture characteristically traverses the posterior wall; however, for the fracture to meet the criteria for an associated wall fracture, the posterior wall must be present as a displaced fragment separate from the posterior column.
Reporting additional data
Reporting the type of fracture as per the Judet and Letournel classification system is important. Also, additional fracture fragments, degree of displacement, and presence of intra-articular fragments should be reported. Finally, 3D images should be reconstructed and archived. These images are helpful for less experienced surgeons or radiologists, and even for experienced observers in the setting of more complex fracture patterns. Techniques that improve fracture visualization include disarticulating the ipsilateral hip (by region-of-interest subtraction) and reconstructing only the fractured hemipelvis. This will also provide the en face view of the acetabulum, as it helps in planning surgery and guiding the surgical approach for reduction.14,22-24
Conclusion
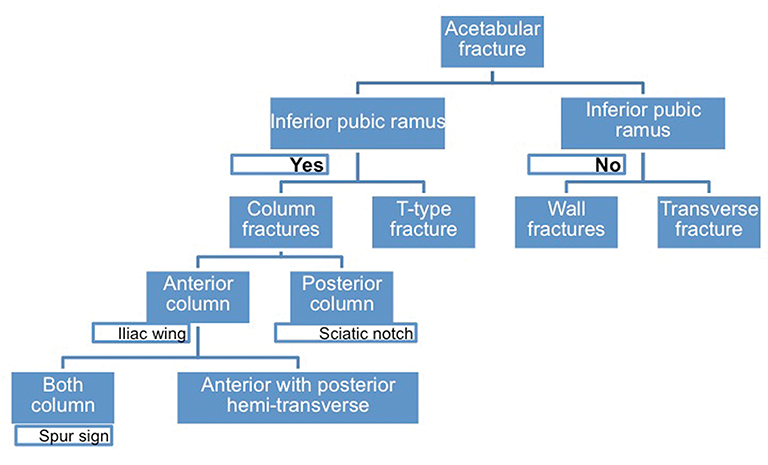
Classifying acetabular fractures according to Judet and Letournel is not easy with radiographs or axial CT images. However, taking a systematic approach as described in the flow chart (Figure 11) can help radiologists reach the correct classification based on axial CT images.
References
- Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am. 1996;78(11):1632-1645.
- Dakin GJ, Eberhardt AW, Alonso JE, et al. Acetabular fracture patterns: associations with motor vehicle crash information. J Trauma. 1999;47(6):1063 - 1071.
- Giannoudis PV, Grotz MR, Papakostidis C, et al. Operative treatment of displaced fractures of the acetabulum: a meta-analysis. J Bone Joint Surg Br. 2005;87(1):2-9.
- Scheinfeld MH, Dym AA, Spektor M, et al. Acetabular fractures: what radiologists should know and how 3D CT can aid classification. Radiographics. 2015;35(2):555-577.
- Alton TB, Gee AO. Classifications in brief: Letournel classification for acetabular fractures. Clin Orthop Relat Res. 2014; 472(1): 35-38.
- Judet R, Judet J, Letournel E. Fractures of the acetabulum: Classification and surgical approaches for open reduction preliminary report. J Bone Joint Surg Am. 1964;46(8):1615-1675.
- Letournel, E. 2007. Acetabulum fractures: classification and management. Orthopedic Trauma Directions. 2007;5(5):27-33.
- Vas WG, Wolverson MK, Sundaram M, et al. The role of computed tomography in pelvic fractures. J Comput Assist Tomogr. 1982;6(4): 796-801.
- Kim JJ, Kim JW, Oh HK. The submuscular sliding plate technique for acetabular posterior wall fractures extending to the acetabular roof. Orthop Traumatol Surge Res. 2014;100(8):967-970.
- Elmadağ M, Güzel Y, Acar MA, et al. The Stoppa approach versus the ilioinguinal approach for anterior acetabular fractures: a case control study assessing blood loss complications and function outcomes. Orthop Traumatol Surge Res. 2014;100(6):675-80.
- Fishman EK. Protocols for helical CT of the musculoskeletal system. Helical (spiral) computed tomography: a practical approach to clinical protocols. New York, NY: Lippincott-Raven; 1998:149-178.
- Bodanapally UK, Shanmuganathan K, Issa G, et al. Dual-Energy CT in hemorrhagic progression of cerebral contusion: Overestimation of hematoma volumes on standard 120-kV images and rectification with virtual high-energy monochromatic images after contrast-enhanced whole-body imaging. Am J Neuroradiol. 2018;39(4):658-662.
- Norman A. The use of tomography in the diagnosis of skeletal disorders. Clin Orthop Relat Res. 1975;107:139-145.
- Burk Jr DL, Mears DC, Kennedy WH, et al. Three-dimensional computed tomography of acetabular fractures. Radiology. 1985;155(1):183-186.
- Jouffroy P, Sebaaly A, Aubert T, et al. Improved acetabular fracture diagnosis after training in a CT-based method. Orthop Traumatol Surg Res. 2017;103(3):325-329.
- Kickuth R, Laufer U, Hartung G, et al. 3D CT versus axial helical CT versus conventional tomography in the classification of acetabular fractures: a ROC analysis. Clinical Radiol. 2002;57(2):140-145.
- Durkee NJ, Jacobson J, Jamadar D, et al. Classification of common acetabular fractures: radiographic and CT appearances. AJR Am J Roentgenol. 2006;187(4):915-925.
- Hunter JC, Brandser EA, Tran KA. Pelvic and acetabular trauma. Radiol Clin North Am. 1997;35(3):559-590.
- Martinez CR, Di Pasquale TG, Helfet DL, et al. Evaluation of acetabular fractures with two-and three-dimensional CT. Radiographics. 1992;12(2):227-242.
- Brandser E, Marsh JL. Acetabular fractures: easier classification with a systematic approach. AJR Am J Roentgenol. 1998;171(5):1217-1228.
- Mack LA, Harley JD, Winquist RA. CT of acetabular fractures: analysis of fracture patterns. AJR Am J Roentgenol. 1982;138(3):407-412.
- Scott Jr WW, Fishman EK, Magid D. Acetabular fractures: optimal imaging. Radiology. 1987;165(2):537-539.
- Fishman EK, Drebin B, Magid D, et al. Volumetric rendering techniques: applications for three-dimensional imaging of the hip. Radiology. 1987;163(3):737-738.
- Matta JM. Operative treatment of acetabular fractures through the ilioinguinal approach: a 10-year perspective. J Orthop Trauma. 2006;20(1):S20-29.
Citation
UK B, M D.Acetabular fractures: A Stepwise approach to identification and classification on 2D computed tomography. Appl Radiol. 2019; (4):17-23.
July 31, 2019