A Rare Case of Lingual Thyroid in a Man
Images

CASE SUMMARY
A 38-year-old man presented with a one-year history of constipation, cold intolerance, and pressure sensation in the lower neck. Physical exam revealed a normal appearance of the posterior wall of the oropharynx with no palpable thyroid gland. Thyroid-stimulating hormone (TSH) was 428 uIU/ml with undetectably low free tetraiodothyronine (FT4). Thyroid peroxidase antibodies were negative. An ultrasound scan of the neck, a contrast-enhanced CT (CECT) scan of the neck, and a thyroid I-123 scan of the neck were obtained.
IMAGING FINDINGS
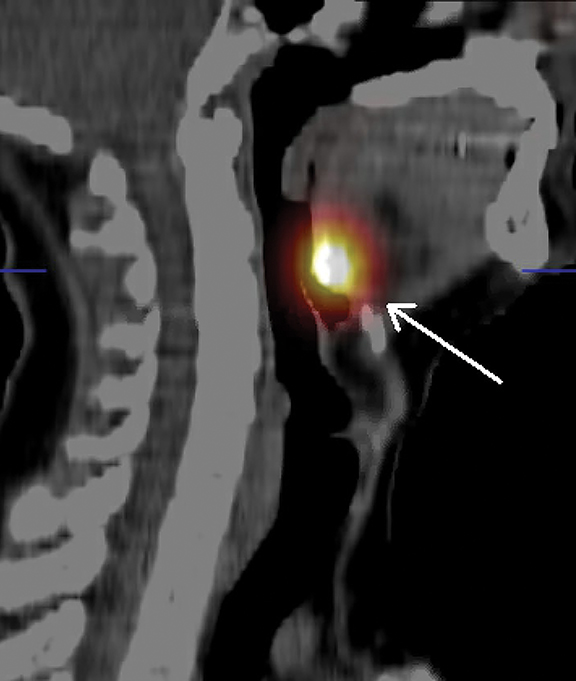
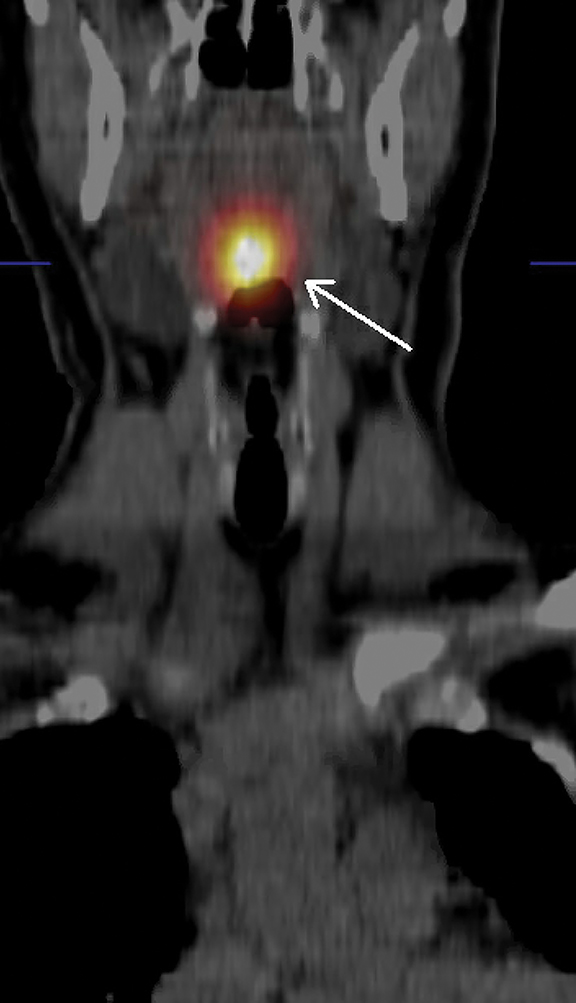
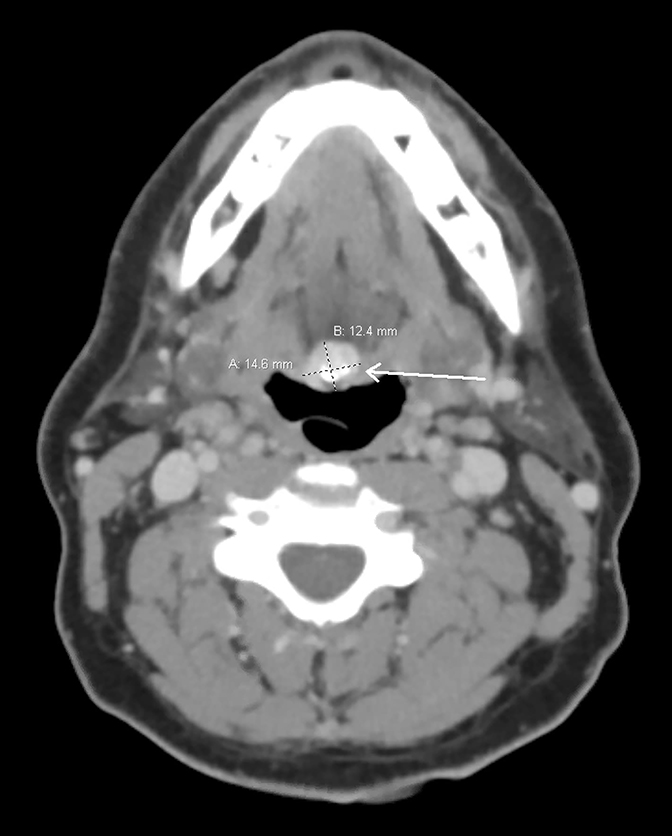
The US showed an absence of thyroid tissue, while the thyroid I-123 scan showed an area of intense radiotracer uptake corresponding to a soft-tissue mass with some calcification posteriorly at the base of the tongue, anterior to the oropharynx at the level of the mandible consistent with lingual thyroid (Figure 1). The CECT showed a densely calcified, hyperdense, contrast enhancing mass in the midline involving the tongue base at the level of the foramen cecum measuring 1.5 cm × 1.2 cm × 1.5 cm with an associated small cystic component (Figure 2).
DIAGNOSIS
Lingual thyroid. Differential diagnoses include lingual thyroglossal duct cyst, lingual abscess, branchial cleft cyst, squamous cell carcinoma of the base of the tongue, and dermoid or epidermoid cyst.
DISCUSSION
Lingual thyroid refers to thyroid tissue at the level of the base of the tongue resulting from development abnormalities during embryogenesis. During the third week of gestation, the thyroid appears as a median diverticulum extending from the foramen cecum at the floor of the first and second pharyngeal pouches. This diverticulum then descends as the thyroglossal tract ventrally and caudally towards the position of the normal thyroid in the anterior neck by the seventh week of gestation. A complete failure of the gland to descend past the foramen cecum results in a lingual thyroid.1
Lingual thyroid, which represents 90% of all cases of ectopic thyroid, was first described in 1869 in a neonate experiencing upper airway obstruction.2 It is a rare congenital anomaly with a prevalence rate between 1 in 100,000 and 1 in 300,000, and reported clinical incidence between 1:4000 and 1:10000.3 Lingual thyroid has a significant female predominance; the female-to-male ratio is 4:1.4 Very few cases of lingual thyroid have been described in male patients.
Lingual thyroids are largely asymptomatic, discovered either incidentally on routine exam or during postmortem studies. Symptoms are related either to clinical hypothyroidism, as in our patient, or to local symptoms from enlargement of the thyroid tissue. Evident hypothyroidism is found in 33% to 62% of patients with lingual thyroid.3
Regional symptoms and signs (dysphagia, dysphonia, dyspnea, hemoptysis, or foreign body sensation) are especially apparent with upper respiratory infections, pregnancy, and other conditions with increased dependence on thyroid hormone and subsequent tissue enlargement.3 Unlike the predominance of papillary carcinoma in the orthotopic thyroid, follicular carcinoma is predominant in lingual thyroid.5,6 Lingual thyroid medullary and anaplastic carcinoma have not been reported.
Multiple radiographic modalities, including ultrasound, scintigraphy, CT, and magnetic resonance imaging (MRI) can be used to diagnose lingual thyroid. Ultrasound of the neck is a noninvasive and cost-effective test that usually demonstrates absence of orthotopic thyroid tissue. A more thorough evaluation of the neck using a low frequency, curved transducer can reveal the size, location, and echogenicity of ectopic thyroid tissue.7
Miller described the sonographic appearance of lingual thyroid as a solid mass with smooth internal texture and low level echogenicity that is similar to normal thyroid parenchyma.8 Thyroid scintigraphy, which utilizes one of the radioisotopes of iodine (usually I-123) or technetium-99m pertechnetate, is considered the modality of choice for identifying ectopic thyroid. It can detect the location, size, and level of activity of any orthotopic and ectopic thyroid tissue. CT and MRI can accurately define the extension and location of any glandular tissue.
Lingual thyroid management varies based on symptomatology and suspicion of malignancy. Asymptomatic and euthyroid patients can be monitored for possible complications. Hypothyroid patients or patients with a mildly enlarged gland causing minimal obstructive symptoms should be started on hormonal suppression therapy to relieve symptoms and reduce the size of the gland.9
Any suspicion of malignancy or the presence of major obstructive symptoms necessitate excision. Surgical removal of the mass can be attempted with an external approach such a trans-hyoid or lateral pharyngotomy, or by performing transoral surgical removal, a newer and safer technique.4 Patients who are not surgical candidates can be treated with ablative radioiodine therapy.10
In our case, fine needle aspiration was not possible given the location of the tissue. The patient underwent transoral robotic lingual thyroidectomy owing to suspicion of malignancy, with the final pathological exam confirming the presence of thyroid tissue, which was negative for malignancy.
CONCLUSION
Lingual thyroid is a rare anomaly among male patients. A high level of suspicion should be present in the setting of clinical hypothyroidism and obstructive symptoms. It is important to note the different radiographic modalities that can be utilized and the different characteristic appearance of lingual thyroid in each study.
REFERENCES
- Fiaschetti V, Claroni G, Scarano AL, Schillaci O, Floris R. Diagnostic evaluation of a case of lingual thyroid ectopia. Radiol Case Reports. 2016. doi:10.1016/j.radcr.2016.04.004
- Choudhury BK, Saikia UK, Sarma D, et al. Dual ectopic thyroid with normally located thyroid: A case report. J Thyroid Res. 2011. doi:10.4061/2011/159703
- Prisman E, Patsias A, Genden EM. Transoral robotic excision of ectopic lingual thyroid: Case series and literature review. Head Neck. 2015. doi:10.1002/hed.23757
- Toso a, Colombani F, Averono G, Aluffi P, Pia F. Lingual thyroid causing dysphagia and dyspnoea. Case reports and review of the literature. Acta Otorhinolaryngol Ital. 2009.
- Massine RE, Durning SJ KT. Lingual thyroid carcinoma: a case report and review of the literature. Thyroid. 2001;11(12):1191.
- Jarvis J. Lingual thyroid: a report of three cases and discussion. South African Med J. 1969;43(1):8–12.
- Lin CY, Yang TL. Lingual thyroid: Ultrasound assessment and diagnosis. J Med Ultrasound. 2014. doi:10.1016/j.jmu.2014.06.005
- Miller JH. Lingual thyroid gland: sonographic appearance. Radiology. 1985. doi:10.1148/radiology.156.1.2988013
- Noussios G, Anagnostis P, Goulis DG, Lappas D, Natsis K. Ectopic thyroid tissue: Anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol. 2011. doi:10.1530/EJE-11-0461
- Iglesias P, Olmos-García R, Riva B, Díez JJ. Iodine 131 and lingual thyroid. J Clin Endocrinol Metab. 2008. doi:10.1210/jc.2008-0909
Citation
D S, A B, D I.A Rare Case of Lingual Thyroid in a Man. Appl Radiol. 2021; (2):42-43.
March 11, 2021