17-year-old male with juvenile recurrent respiratory papillomatosis
Images



Case summary
A 17-year-old male with known juvenile recurrent respiratory papillomatosis, due to HPV (human papilloma virus) types 6 and 11, presented with exacerbation of cough and dyspnea. He had undergone several endoscopic procedures for resection and laser ablation of the papillomas and had been treated with intravenous cidofovir, an antiviral drug, with some improvement. However, he recently developed mediastinal and right hilar adenopathy, which was biopsied, revealing follicular hyperplasia without malignancy. He is being followed with multidetector computed tomography (MDCT) scans of the chest and airway to evaluate the status of his tracheobronchial papillomas, pulmonary cavities, and bronchiectasis.
Imaging findings
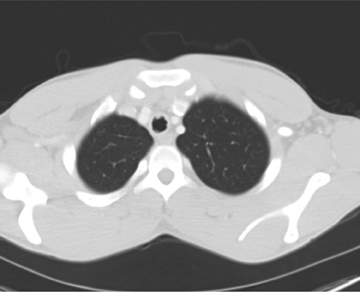
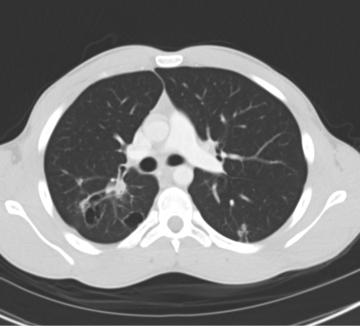
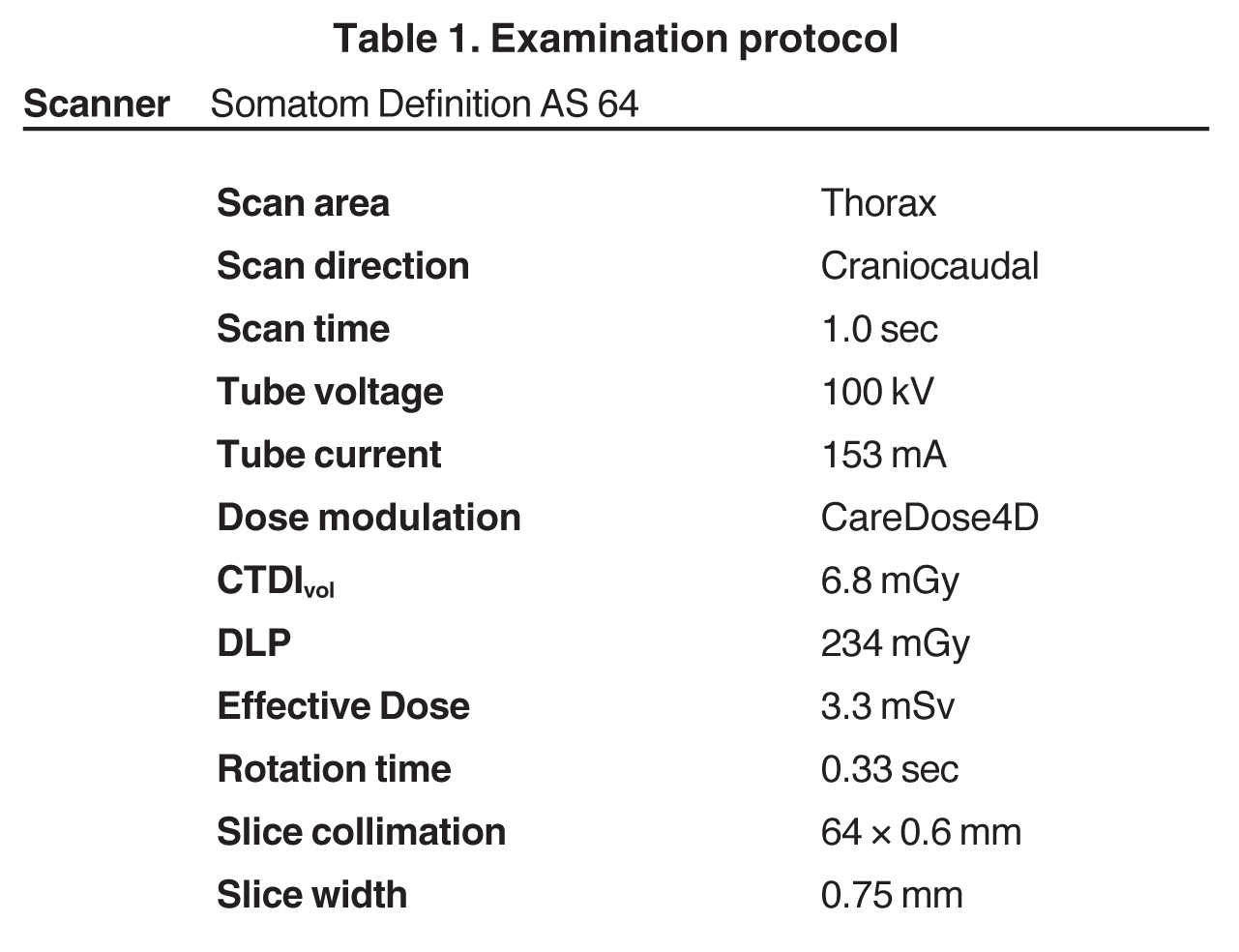
A CT examination was performed with a Somatom Definition AS 64 scanner (Siemens, Erlangen, Germany). The CT scan revealed multiple polypoid masses protruding into the lumen of the trachea, consistent with tracheal papillomatosis (Figure 1). The largest of the lesions measured approximately 6 mm. CT also showed a 5.0 x 3.0 cm right infrahilar mass with consolidation in the right lower lobe distal to this mass, representing postobstructive pneumonitis (Figure 2). Multiple cavitary lesions with thick, irregular walls and multiple nodules were also observed in both lungs (Figure 3 and 4).
Diagnosis
Recurrent tracheobronchial papillomatosis with pulmonary involvement due to HPV types 6 and 11.
Discussion
Recurrent respiratory papillomatosis is the most common benign tumor of the larynx in childhood, caused by infection with human papillomavirus (HPV), most commonly types 6 and 11.1,2 The exact mode of transmission is unclear and is likely variable depending on the age of the patient at presentation. In neonates and children, the likely route is direct exposure of the neonate to the virus in the birth canal during delivery. Among adults, the disease may be associated with oral-genital contact.1 Affected children usually present with hoarseness and occasionally with stridor, cough, or recurrent pneumonia. The disease is characterized by benign epithelial tumors of the airway, which most frequently are limited to the laryngeal and subglottic areas. Involvement of lower airways and lungs is rare. In 4% to 17% of patients, the distal trachea and bronchi are involved, and in <1% to 5% of patients, there is pulmonary involvement.3 Malignant transformation into squamous cell carcinoma occurs in 2% to 3% of cases, usually affecting older children or adolescents.4
Chest radiography is the initial examination to diagnose pulmonary involvement. If the chest examination is abnormal, CT is the imaging examination to assess the extent and stability of disease. The CT findings of airway involvement are tracheal irregularity, multiple nodules attached to the tracheal-bronchial walls, and bronchiectasis secondary to bronchial obstruction and chronic infection. Postprocessing techniques, such as multiplanar reconstructions (MPR) and volume rendering (VR), as well as virtual bronchoscopy (VB), are useful to improve visualization and localization of lesions. In this case, the MPR showed the lesions attached to the tracheal wall. The VB demonstrate sessile papillomas.
The characteristic CT findings of lung involvement are multiple solid and cystic nodules, predominantly in the lower lobes.5 As the nodules grow, the blood supply to the center of the nodules is lost and central necrosis occurs. The cystic nodules may enlarge and form large cavities with thick or thin walls. Enlargement of a previously described lesion and mediastinal lymphadenopathy should increase the suspicion of malignancy.6 In addition, parenchymal complications, such as pneumonia, abscess, and atelectasis, can be seen.
Conclusion
We present the CT findings of juvenile recurrent respiratory papillomatosis with pulmonary involvement. CT provides excellent characterization of anatomy and can help plan bronchoscopy and tumor resection. Serial CT studies are mandatory because of the possibility of malignant transformation of papillomas. Current CT scanners provide high levels of anatomic detail with low radiation doses.
References
- Larson DA, Derkay CS. Epidemiology of recurrent respiratory papillomatosis. APMIS. 2010;118:450-454.
- Dickens P, Srivastava G, Loke SL, Larkin S. Human papillomavirus 6, 11, and 16 in laryngeal papillomas. J Pathol. 1991;165:243–246.
- Kramer SS, Wehunt WD, Stocker JT, Kashima H. Pulmonary manifestations of juvenile laryngotracheal papillomatosis. AJR Am J Roentgenol. 1985;144:687–694.
- Gerein V, Rastorguev E, Gerein J, et al. Incidence, age at onset and potential reasons of malignant transformation in recurrent respiratory papillomatosis patients: 20 years experience. Otolaryngol Head Neck Surg. 2005;132:392–394.
- Prince JS, Duhamel DR, Levin DL, et al. Nonneoplastic lesions of the tracheobronchial wall: Radiologic findings with bronchoscopic correlation. Radiographics. 2002;22:S215-S230.
- Frauenfelder T, Marincek B, Wildermuth S. Pulmonary spread of recurrent respiratory papillomatosis with malignant transformation: CT findings and airflow simulation. Eu J Radiol Ex. 2005;56:11-16.
Related Articles
Citation
17-year-old male with juvenile recurrent respiratory papillomatosis. Appl Radiol.
July 27, 2011