Uterine artery embolization
Images

This case is brought to you by Guerbet, LLC.
Case Summary
A 49-year-old perimenopausal female presented with a history of abnormal uterine bleeding, pelvic pain, prolonged men struation, uterine fibroids, and metabolic syndrome. Pelvic ultrasound demonstrated increased size of numerous fibroids, including subserosal and intramural subtypes. The largest intramural fibroid measured 3.0 x 3.0 cm. The remaining sonographic examination was unremarkable, aside from a stable 1.7 cm right ovarian cyst. Endometrial biopsy was negative for malignancy; the patient had previously trialed intrauterine device hormonal therapy without symptom relief. She was then presented with such treatment options as uterine artery embolization (UAE), hysterectomy, and hormone therapy.1 The patient elected to be treated with UAE and was referred to interventional radiology and surgery.2
Diagnosis
Symptomatic uterine fibroids
Image Findings
The patient underwent UAE utilizing the left radial artery approach.3 A 4/5 Fr slender sheath was placed into her left radial artery, followed by delivery of vasodilator cocktail. The bilateral iliac arteries were cannulated with a 5 Fr Soft-Vu JB-1 catheter (Angiodynamics, Amsterdam, Netherlands). Angiography demonstrated tortuous and engorged bilateral uterine arteries supplying the leiomyomatous uterus.
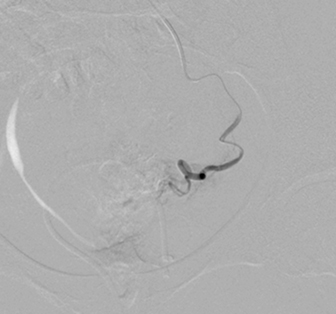
After careful image-guided planning, the left uterine artery was selected via a 130-cm, 2.8 Fr SeQure® microcatheter (Guerbet, Roissy CdG, France). Initial arteriogram re-demonstrated tortuous and dilated uterine artery without evidence of collateral supply or accessory cystic artery. Bland embolization via 300-500 um Embospheres (Merit Medical, South Jordan, UT) was administered via the left uterine artery. Post-embolization angiography demonstrated complete stasis without evidence of contrast reflux (Figure 1).
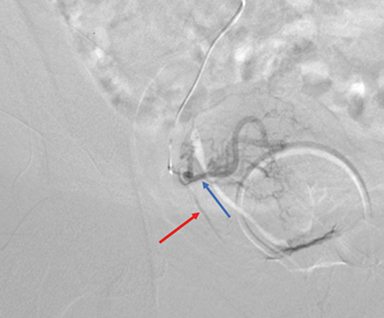
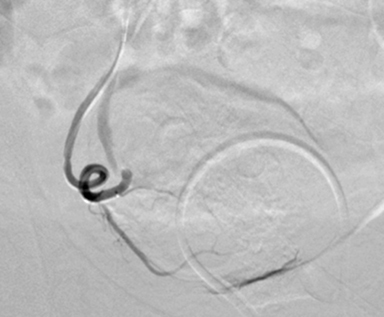
The right uterine artery, was then selected using the SeQure® microcatheter in similar fashion. However, this angiogram demonstrated an additional single-vessel supply to the inferior margin of the bladder, most consistent with an accessory cystic artery (Figure 2). The SeQure® microcatheter was easily negotiated beyond the accessory cystic artery takeoff, through the tortuous right uterine artery. The right uterine artery was then embolized in similar fashion with exclusion of the accessory vesicular artery, presumably via the unique flow-directed methodology of the SeQure® microcatheter. Complete stasis of the right uterine artery was noted status post-embolization, with complete preservation of the accessory cystic artery (Figure 3).
Discussion
The SeQure® microcatheter was designed to assist with, and limit reflux during, flow-directed embolization procedures. In this case, the microcatheter was employed to deliver embolic agents to the bilateral uterine arteries in the setting of symptomatic fibroids.2 Specifically, the microcatheter was able to isolate the right uterine artery and completely exclude the accessory cystic artery without requiring additional interventions, such as balloon occlusion, etc. This case demonstrates additional use of a microcatheter for excluding unwanted, nontargeted embolization in the appropriate clinical setting.
The SeQure® microcatheter provided excellent tracking ability through the uterine arteries in a well-controlled fashion without causing spasm of the associated artery.
Conclusion
Uterine artery embolization can be performed with a SeQure® microcatheter to successfully manage patients with symptomatic fibroids.
References
- Mortensen C., et al. Prospective study on total fluoroscopic time in patients undergoing uterine artery embolization: Comparing transradial and transfemoral approaches. Cardiovasc Interv Radiol.2018: 42(3) 441–447. doi:10.1007/s00270-018-2100-3.
- Gupta JK., et al. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database of Systematic Reviews. 2012. doi:10.1002/14651858.cd005073.
- Hirst A., et al. A Multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids. The HOPEFUL study. Health Technol Assess. 2008; 12(5). doi:10.3310/hta12050.
Citation
A R,. Uterine artery embolization. Appl Radiol. 2019;(5):30-31.
September 25, 2019