The Role of Interventional Radiology in Acute Trauma
Images


With continued advances in angiography and transcatheter techniques and procedures, interventional radiology (IR) is playing an increasingly larger role in the management of patients suffering acute traumatic injuries.
At a Level One trauma center like that at the University of Chicago, IR is invaluable in treating vascular injuries via transcatheter embolization and endovascular repair, specifically in major arterial injuries. In addition to standard angiography and transcatheter imaging technologies, the institution’s department of vascular and interventional radiology has implemented a state-of-the-art 4D CT interventional suite (Canon Medical Systems USA, Inc.). The 4D CT solution contains an advanced ceiling-mounted C-arm fluoroscopy unit combined with a moveable CT scanner on sliding rails within the same room. CT angiography is one of the most effective and efficient ways to diagnose acute traumatic injuries. The combination of imaging modalities with interventional radiologists ideally qualified to manage trauma patients allows for optimal care by reducing the time from diagnosis to treatment and avoiding surgical morbidity.
One of the most important benefits of this approach is that multiple sequential procedures and/or longer, more complex, stepwise procedures can be performed in the same room, without transporting the patient between the CT scanning room and the IR suite. This allows the patient to remain in the same position with minimal disruption in workflow.
Many complex embolization procedures require time and expert technique to optimally access the most proximal location of vascular extravasation. Moving the CT scanner to the patient preserves the room and patient set-up and nearly eliminates the risk of losing vascular access.
Additionally, 4D CT allows for rapid-sequence, targeted CT imaging, which can provide superior anatomic visualization of the injured area, including surrounding soft tissues, versus predominately only the vasculature, as seen with conventional angiography. These real-time images can also be reformatted and reconstructed rapidly, including 3D volumetric reconstructions. By obtaining greater knowledge of the region of interest and the 3D course of regional vasculature, interventional radiologists gain a superior roadmap compared to traditional fluoroscopy and 2-D DSA images used in conventional angiography. This improvement, from a technical standpoint, can greatly reduce procedure duration, treatment efficiency, and radiation dose.
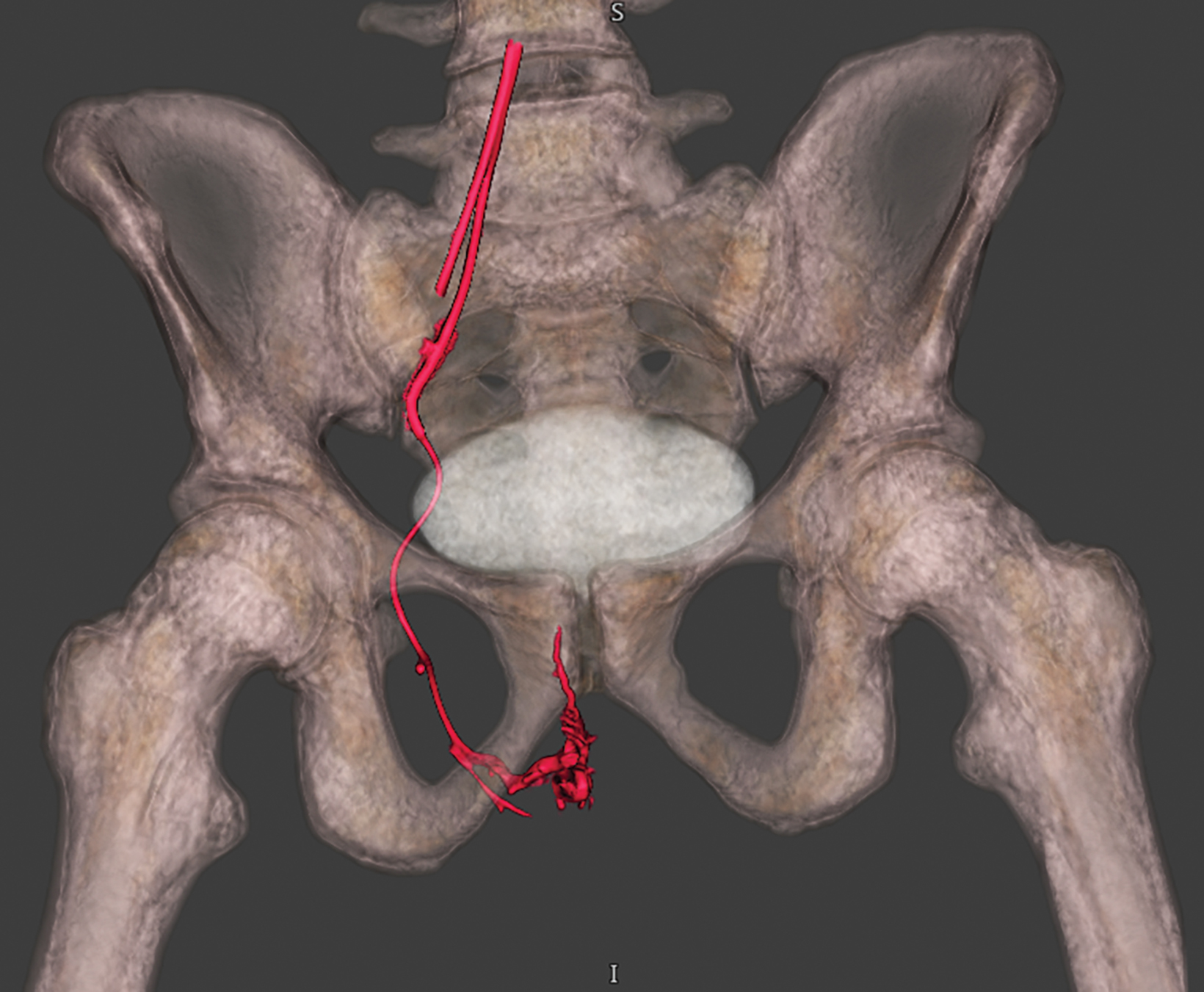
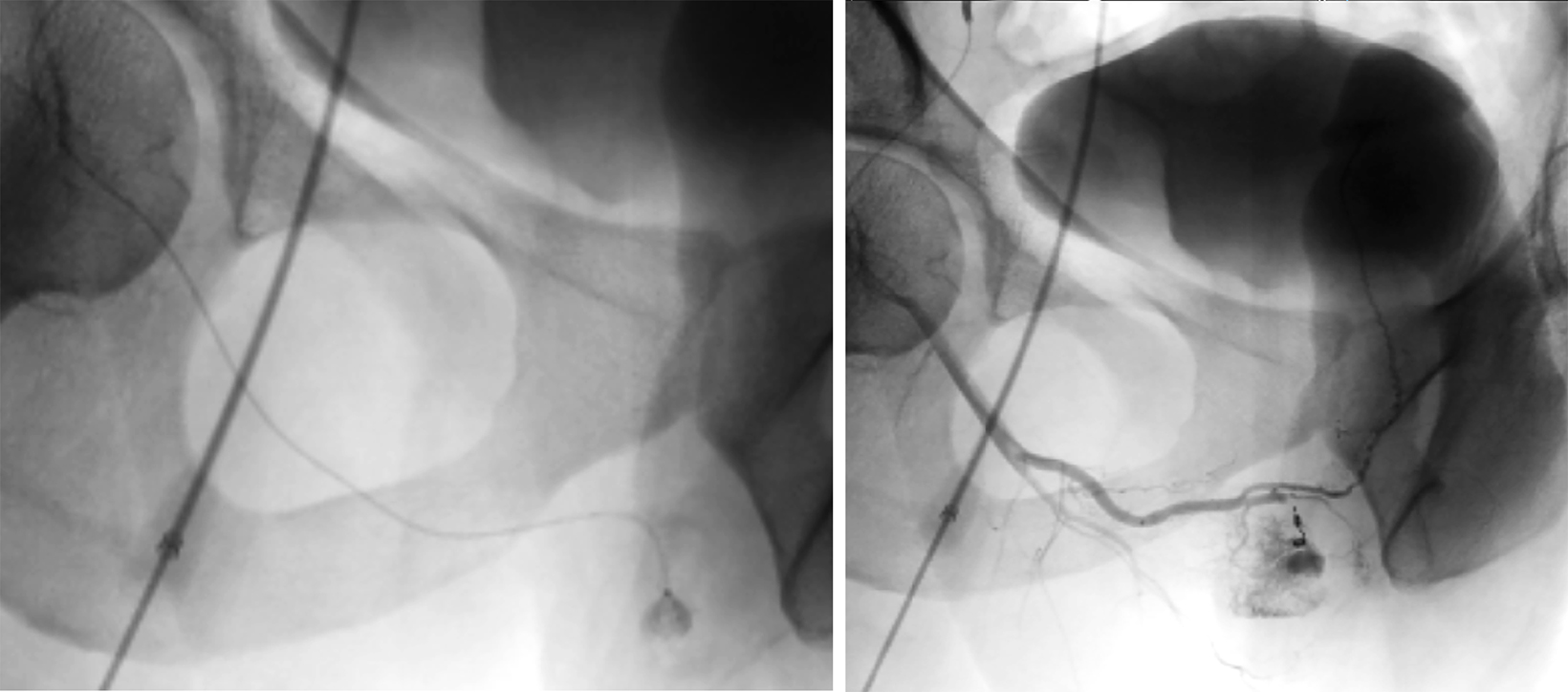
See one example of the utility of 4D CT and rapid generation of 3D reconstructions accompanying this article. This example highlights the role of hybrid CT angiography in diagnosing and treating a high-flow, pudendal arterial cavernous fistula resulting in high-flow priapism.
In addition to improving the procedure roadmap itself, intermittent CT scans can be performed at the region of interest to continuously monitor procedure effectiveness, improve patient safety, minimize complications, and increase efficiency. There are also drastic technical improvements when using CT compared to conventional fluoroscopy. For example, the CT scanner can be operated in multiple phases, including noncontrast, arterial-weighted, and portal venous. This technical availability within the angiography suite allows for delineation of the injury’s exact location, composition, type of bleed, and any adjacent injuries. In addition, CT can help alleviate simple diagnostic dilemmas frequently seen on conventional fluoroscopy, such as impaired/obscured visualization of the region of interest resulting from overlying bowel gas.
While this example illustrates just one aspect of the impact and utilization of 4D CT, our experience more broadly has evidenced improved efficiency and quality of care within the vascular and interventional radiology department, specifically with respect to management of acute trauma.
Indeed, 4D CT has innumerable other applications, including renal artery aneurysm embolization, endoleak repair, CT-guided biopsy, cryoablation, Yttrium-90 mapping, and many more.
Reference
https://us.medical.canon/download/gest-vl-cs-4dct-case-workflow