Study Finds iFR and FFR Equally Safe to Diagnose and Treat Heart Disease
Images
A longitudinal analysis from the National Swedeheart Quality Registry of more than 42,000 patients undergoing coronary procedures showed no difference between instant wave-free ratio (iFR) and fractional flow reserve (FFR) in major adverse cardiac events (MACE). The analysis, “Long-term Safety of Revascularization Deferral Based on Instantaneous Wave-Free Ratio or Fractional Reserve,” compares patient outcomes using iFR and FFR in the diagnosis and treatment of heart disease and was presented in a late-breaking science session at the Transcatheter Cardiovascular Therapeutics (TCT) 2023 meeting.
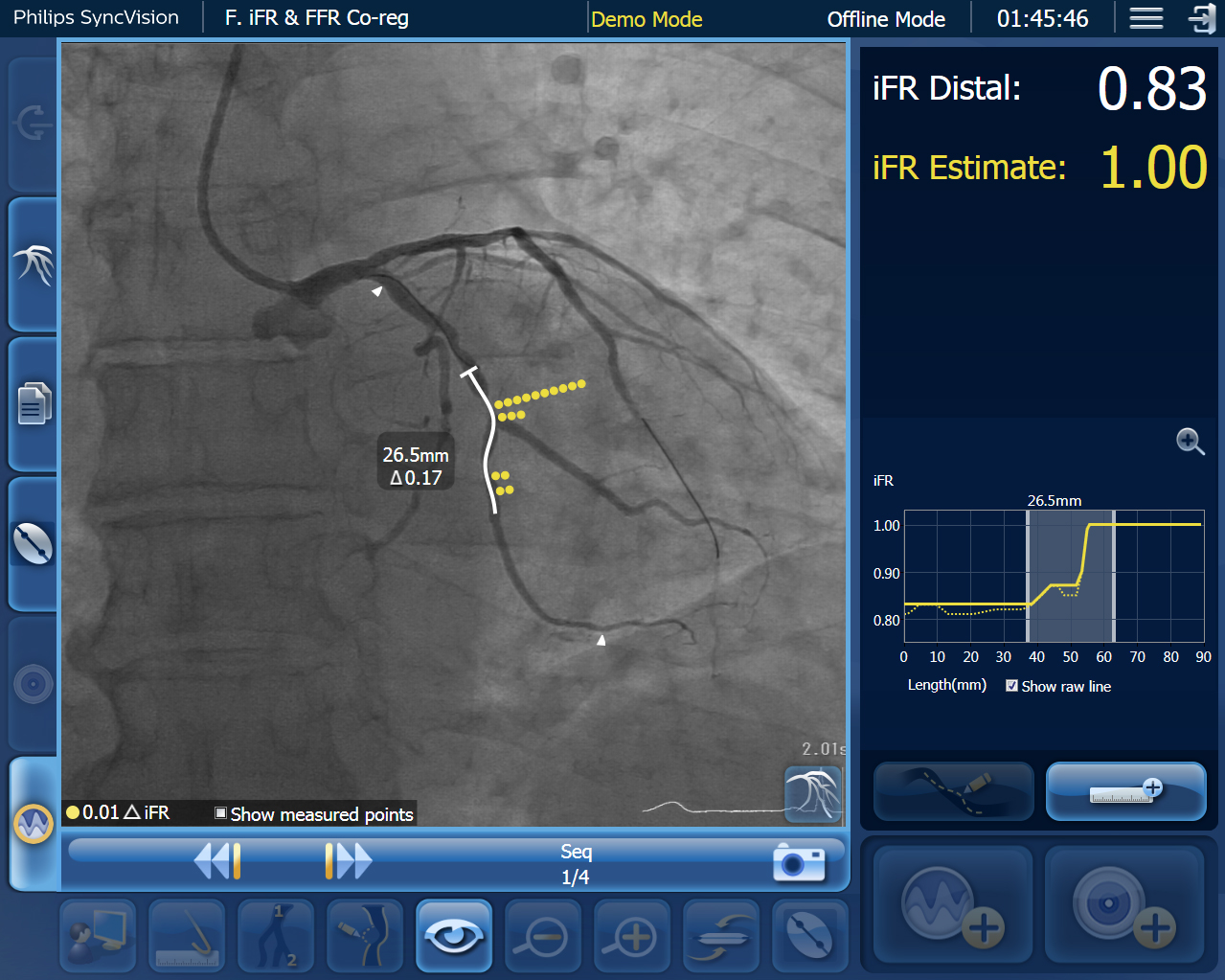
Royal Philips is the provider of iFR, a pressure-derived index that is used to assess coronary blockages during interventional procedures without the use of hyperemic agents.
“These new findings once again confirm the safety of iFR. We continue to see that iFR-guided treatment offers consistent outcomes, reduces costs, and provides a better patient experience,” said Dr Matthias Götberg, Department of Cardiology, Clinical Sciences, Lund University, Sweden, who presented the results. “The data from this new analysis provides additional confidence in the safety of iFR for physicians.”
In the previously published analysis of the five-year outcomes of the randomized trial iFR-SWEDEHEART, results found iFR and FFR to be equally safe and effective with respect to risks for MACE. The cumulative MACE risks for each group differentiated by 1.6% (iFR: 21.5%, FFR: 19.9%, HR 1.09 (95% CI: 0.90-1.33 at 5 years). There was no difference in risk for death, heart attack or new revascularization.
The results presented today from the SWEDEHEART registry revealed that patients in the iFR group had more risk factors compared with the FFR group but when adjusted for known confounders there was no difference in 5-year MACE between patients who underwent iFR or FFR-guided revascularization (32.2% vs. 31.3%, adjusted HR 0.99, 95%CI 0.93–1.05, p=0.65). Furthermore, the outcome was similar in the individual components of MACE (death, heart attack, new revascularization) as well as in both deferred and treated subgroups.
iFR is considered the gold standard for hyperemia-free physiologic assessment for measuring pressure in diagnostic and interventional procedures. Similar to FFR, clinicians use these tools coupled with angiographic images to assess coronary blockages. However, by avoiding administrating a hyperemic agent, patient discomfort can be reduced by 95.7% and enables iFR to detect disease processes downstream from the major blood vessels.
Only Philips iFR has a Class IA recommendation by the American College of Cardiology, American Heart Association, Society for Cardiovascular Angiography & Interventions and European Society of Cardiology.
“We are confident in our pursuit of innovation to improve outcomes and ensure patient safety. The data continues to demonstrate the benefits of iFR-guided treatment to reduce costs and improve outcomes,” said Chris Landon, General Manager, Philips Image Guided Therapy Devices. “iFR technology is unique to Philips, and we are proud to offer the global gold standard treatment for patients with ischemic heart disease.”
Related Articles
Citation
Study Finds iFR and FFR Equally Safe to Diagnose and Treat Heart Disease. Appl Radiol.
October 27, 2023